info@biomedres.us
+1 (502) 904-2126
One Westbrook Corporate Center, Suite 300, Westchester, IL 60154, USA
Site Map

Received: January 06, 2018; Published: January 17, 2018
*Corresponding author: Abhimanyu Mohanta, Biju Pattnaik Clollege, Singda, Mayurbhanj, Odisha, India- 757039
DOI: 10.26717/BJSTR.2018.02.000667
Dental fluorosis is a chronic fluoride –induced condition in which an excess of fluoride is incorporated in the developing tooth enamel and disrupt the enamel formation of the tooth. Prevalence of dental fluorosis due to high levels of fluoride in drinking water is an endemic global problem. Although, definite mechanism of dental flourosis is yet to be confirmed, hypomineralization of teeth enamel is the real fact and so the teeth enamel become more porous and softer than the normal counterparts. More exposure to the fluoride, greater is the rate of dental fluorosis. Also, children with mild dental fluorosis had lower IQ than those without dental fluorosis demands further investigation.
Keywords: Fluorosis; Endemic; Enamel; Ameloblast; Intelligent Quotient (IQ)
Dental fluorosis is one of the growing dental public health problems in many parts of the globe. Prevalence of dental fluorosis seems to be increasing in populations especially those with high levels of fluoride in drinking water. It is more common in hilly areas where natural existence of fluoride is dominant [1]. Dental fluorosis is a chronic fluoride –induced condition in which an excess of fluoride is incorporated in the developing tooth enamel and disrupt the enamel formation of the tooth. Children in the age group of 0 to 12 years are the most prone to fluorosis as their body tissues are in formative growth stage during this period [2]. Being an anti-cariogenic agent, fluoride has been used in tooth paste, mouth wash, chewing gum, and some prescribed diet to treat dental caries. However, cumulative exposures to these things are reported to enhance the dental fluorosis [3]. In the present review, pathophysiological aspect of endemic dental fluorosis and its association with the intelligent quotient (IQ) of the children were briefly highlighted.
Clinical, experimental, and review reports were searched in a number of bibliographic databases for scientific literature, using the search phrase “dental fluorosis’, ‘epidemiology of dental fluorosis’ and ‘dental fluorosis and IQ’.”
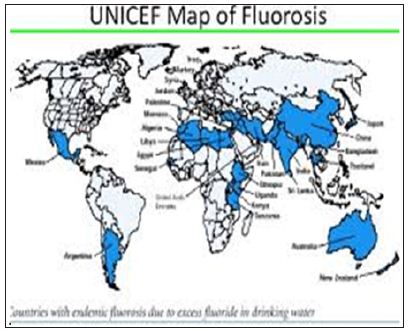
Due to the universal presence of fluoride in water, soil and the atmosphere it is not surprising that humans are exposed to various levels of fluoride intake, not only through food and water, but in industrial and pharmaceutical products and other sources. Water-borne fluoride, however, has been said to represent the largest single component of this element’s daily intake, except where unusual dietary patterns exist. World Health Organization (WHO) has recommended that the permissible limit of fluoride concentration in drinking water is 1.5mg/l. Dental fluorosis is an acute, chronic and endemic problem worldwide (Figure 1). Epidemiological studies on fluorosis have been reported from various regions of the world including Africa [4-7], Saudi Arab [8,9], India [10], China [11], Pakistan [12], Tanzania [13], Brazil [14], Kenya [15] Taiwan [16], and Malawi [17]. Chinese data on endemic fluorosis from 1990 to 2000 indicate that the state of the fluorosis had been well under control during these ten years. The prevalence of water based fluorosis in Huabei, Huadong and Xibei was declining, while the prevalence of fluorosis in Dongbei was increasing. Also the non-water-based fluorosis was reported to have been rising in west China [18]. Recently, Siddiqui et al. have reviewed and reported that mild to very mild fluorosis are very dominant in Saudi Arabian population except in Riyadh where severe fluorosis was also experienced by many [19].
Figure 1: Endemic dental fluorosis worldwide.
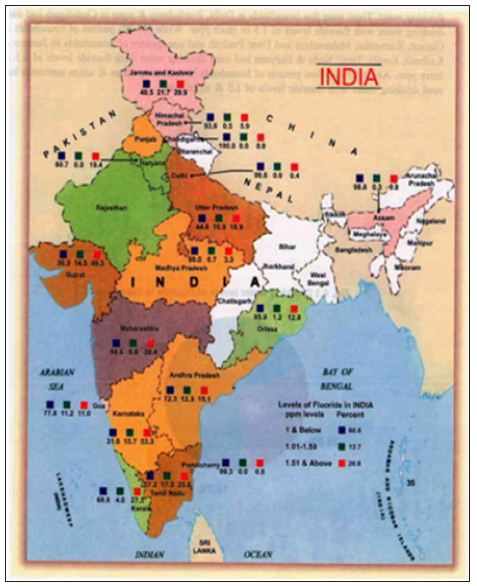
Under National Oral Health Survey & Fluoride Mapping 2002-2003, almost 19 states and Union Territories of India were covered and are reported to be highly affected with endemic fluorosis (Figure 2). High incidence of endemic fluorosis in India is due to the fact that large areas of the country contain high level of fluoride in the drinking water sources [20]. By way of multiple epidemiological studies, Dean and Elvove have established the fact that there was a close link between dental fluorosis and excessive fluoride in the drinking water. They have concluded that fluoride at the level of 1 ppm in the drinking water would no doubt reduce dental caries, but having minimal detrimental effects with dental fluorosis [21,22]. Besides the fluoride in the drinking water, factors such as temperature [23-25], altitude of residence [26,27], diet and nutrition [28,29], and dental products [30-32] have been reported to influence dental fluorosis. It has been well observed that some children swallow more fluoride from toothpaste alone than is recommended from all sources combined. Ingesting toothpaste during childhood is a major risk factor for dental fluorosis, and can also cause symptoms of acute fluoride toxicity (e.g., nausea, vomiting and stomach pain, etc) [33].
Figure 2:Fluoride concentration in drinking water in the different States of India.
On the basis of degree of severity of the mottled enamel, which were associated with varying levels of fluoride in the drinking water defects Dean [34] has classified the dental fluorosis into six classes (Tables 1 & 2).
Table 1: Diagnostic criteria and weighting system for Dean’s Index.
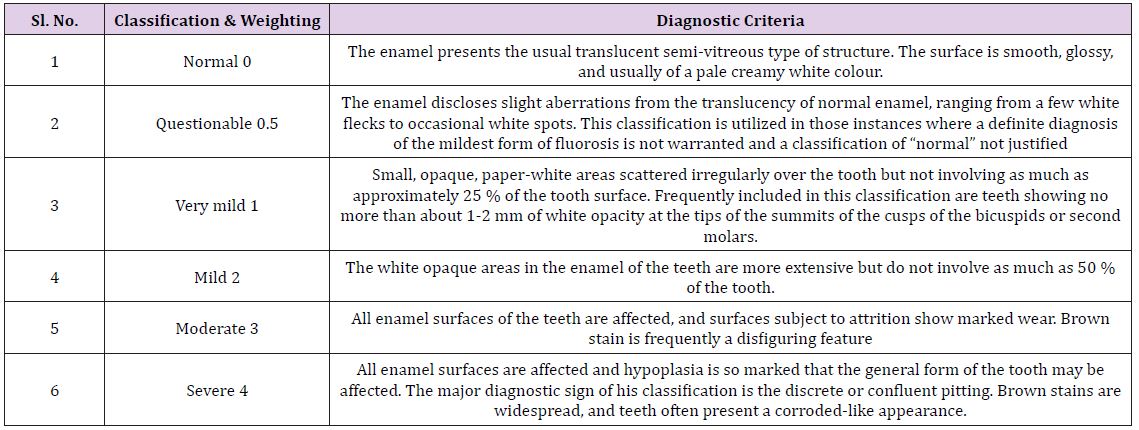
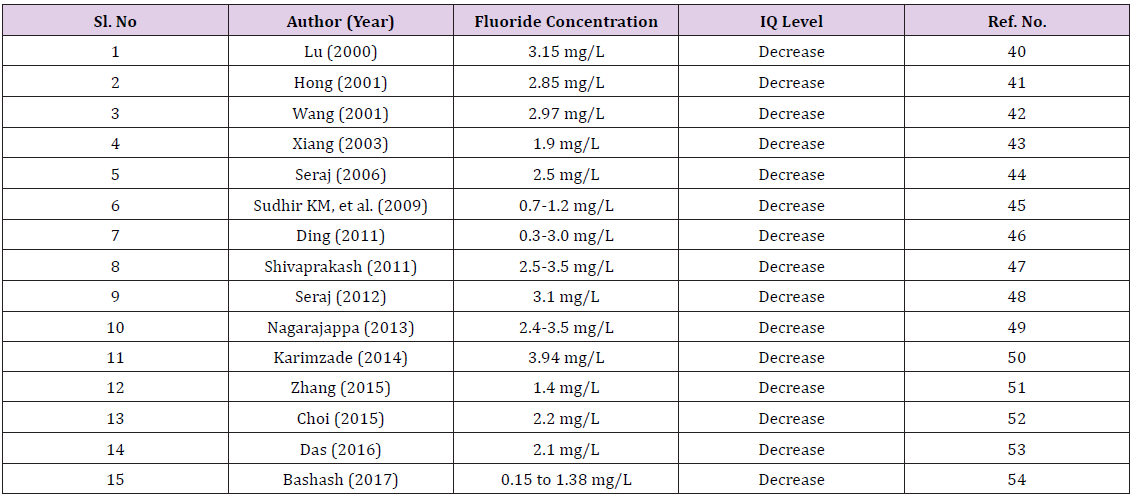
Table 2: Status of Inteligent Quotient (IQ) Level of children at different concentration of fluoride level in drinking water
Dental fluorosis is a sign of fluoride toxicity and can range from very mild to severe. Clinically, it is characterized by staining and pitting of the teeth. In more severe cases, the entire enamel may be damaged and lost. During formative stage, intake of fluoride content drinking water enamel formation is disturbed and ultimately gets hypo-mineralised at its maturation. The prevalence of dental fluorosis is dependent upon the fluoride intake in the early stage of life [35]. The development of fluorosis is also highly dependent on the dose, duration, and timing of fluoride exposure. The risk of enamel fluorosis is lowest when exposure takes place only during the secretory stage, but highest when exposure occurs in both secretory and maturation stages [36]. Enamel is produced by specialized epithelial cells called ameloblasts. The chief function of an ameloblast is to support the growth of a single hydroxyl-apatite enamel rod by secreting scaffold proteins during the secretory stage, in which the rods growth in length, and then removing these proteins during the maturation stage, in which the rods thicken [37]. Fluorosis occurs when fluoride interacts with mineralizing tissues, causing alterations in the mineralization process.
In dental enamel, fluorosis causes subsurface hypomineralization or porosity, which extends toward the dentinal-enamel junction as severity increases. This subsurface porosity is most likely caused by a delay in the hydrolysis and removal of enamel proteins, particularly amelogenins, as the enamel matures. At the early maturation stage, the relative quantity of amelogenin protein is increased in fluorosed enamel in a dose-related manner. This appears to result from a delay in the removal of amelogenins as the enamel matures [38]. Although, definite mechanism of dental flourosis is yet to be confirmed, current knowledge on ameloblast function during enamel formation may help to understand the same. Previously it was demonstrated that fluoride induces phosphorylation of the alpha subunit of eukaryotic initiation factor 2 (eIF2ᾳ) ribosomal components, which significantly decreases protein synthesis. This occurs during the maturation stage of development when proteins are normally removed from the hardening enamel. Megan et al. have recently hypothesized a potential mechanism in which excess fluoride results in increased protein levels and softened enamel via decreased protease secretion during the maturation stage.
According to them phospho-eIF2ᾳ mediated inhibition of protein production induced by intracellular fluoride results in decreased secretion of the enamel protease kallikrein-4 (KLK4) during the enamel maturation phase. This in turn results in decreased protein breakdown and higher protein content within the enamel matrix [39]. At low concentration fluoride gets incorporated ions into the hydroxyapatite crystals of enamel which increases hardness and reduces demineralization, thereby prevents caries formation. Excess fluoride, however, has a detrimental effect on developing enamel, resulting in opaque mottling, pitting and, in severe cases, makes enamel porous, soft and severely demineralised. The fluorotic enamel are found to be hypomineralized with, increased levels of protein content when compared to the nonfluorosed enamel [40,41].
Findings evidence that fluoride exposure during the early years of life can damage a child’s developing brain. Researchers from different countries have reported that IQ level of the children was seriously affected by water fluoride even at lowest concentration! Almost all the authors have concluded that overall IQ levels in children’s exposed to high fluoride level were significantly lower than the low fluoride areas and Children with mild dental fluorosis had lower IQ than those without dental fluorosis [42-55].
Dental fluorosis is not merely a cosmetic problem but a serious condition that affects the aesthetic, emotional, social, and even psychological aspects of an individual‘s life. Whatever it may be the source, fluoride has a detrimental effect on teeth enamel leading to premature loss of teeth at large, Furthermore, how does dental fluorosis affect the central nervous system and lower the IQ level among children needs further investigation.


























