 Review Article
Review ArticleABSTRACT
The ongoing pandemic, caused by SARS-CoV-2, has dramatically impacted the world for the past two and a half years. Much effort has been focused on the prevention and treatment of this disease, along with the emergence of dominant variants. Here, we review the progress of current research on this virus and its variants, with a focus on the new Omicron variant. With the recent lockdowns in areas like Shanghai, attention needs to be paid to the psychological impact of the pandemic on the residents, especially adolescents.
Introduction
COVID-19, a highly contagious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), produced its first outbreak in Wuhan, the capital of Hubei province in China in December 2019, when it coincided with the Chunyun period, a period of high traffic around the Chinese Lunar New Year. It was very contagious and had no effective treatment, such that even after the lockdown of Wuhan, it still spread to the whole world and infected a huge percentage of the population, inflicting death, which led the World Health Organization to proclaim it a pandemic. As of today (June 16, 2022), according to the Johns Hopkins Coronavirus Resource Center, SARS-CoV-2 has caused 537,601,288 cases of infection worldwide, and 6,315,704 deaths.
Two and a half years after its outbreak, although dramatic efforts have been made to contain the pandemic, including vaccines, mask mandates, screening, testing, isolation (such as the recent Shanghai lockdown), the pandemic is still ongoing. SARS-CoV-2 has not just impacted health, it has also impacted the economy and almost every area of life worldwide. It has led to a sharp increase in unemployment, disruptions in the supply chain, like a baby formula shortage, and a surge in inflation, which is the highest it has been in the past four decades in the US [1] .On the other hand, huge progress has been made in the knowledge of the virus, as well as methods of prevention, detection, diagnosis, and treatment. At the same time, the pandemic, as well as responses to it, have revealed problems that have not been heavily researched before, like the psychological impact of isolation or even lockdown on adolescents, and more research and efforts are needed to address these problems. Here we provide some updated information focused on the virus and its variants, and we hope this pandemic will end in the near future.
SARS-CoV-2
Coronaviruses (CoVs) are a group of RNA viruses that belong to the family Coronaviridae within the order Nidovirales. They are enveloped viruses, with a single-stranded RNA genome, and a nucleocapsid. They can infect other vertebrates, including bats, birds, mice and other animals, in addition to human beings [2]. They can cause human respiratory infections, and the risk varies significantly. About 15% of cases of the common cold is caused by a coronavirus [3]. Till now, there have been three strain of coronavirus which have a very high morbidity and mortality in humans. In 2002- 2004, severe acute respiratory syndrome coronavirus (SARS-CoV or SARS-CoV-1) caused an outbreak in China, spread to 32 different countries and regions, and caused more than 8000 infections and 919 related deaths with a case fatality rate (CFR) of 11% [4]. Middle East respiratory syndrome coronavirus (MERS-CoV) is a virus transferred from dromedary camels. MERS-CoV has been identified in several countries in the Middle East, Africa and South Asia. It was responsible for 2468 cases and 851 deaths with a CFR of 37.2% [5]. MERS-CoV did not fully adapt to human transmission, and most of the cases are due to spillover from camels [6]. In comparison with the other two coronaviruses, SARS-CoV-2 appears to be much more contagious and infectious. But the CRF is much lower than those of SARS-CoV-1 and MERD-Cov [7].
As for SARS-CoV-2, through comparing the data of the whole genomic sequence, the Wuhan strain is considered a new strain of β coronavirus with approximately 79% genetic similarity to SARS-CoV [8]. As it has a 96% similarity to a bat coronavirus, it is suspected to originate from bats [8-9]. SARS-CoV-2 has some features that allowed it to spread quickly and claim millions of lives. Its spike protein is coated with glycans, which help it evade the human immune system. The binding of the spike protein of the virus to the angiotensin-converting enzyme 2 (ACE2) of the host cell is necessary for both SARS-CoV-1 and SARS-CoV-2 for virus infection. It has been shown that SARS-CoV-2’s binding is 2-4 times stronger than that of SARS-CoV-1. For the merge of viral and cell membranes, both of these viruses use TMPRSS2 or cathepsin L (host protease). TMPRSS2, which is expressed abundantly on the outside of respiratory cells, is the faster route in, and SARS-Cov-2 uses TMPRSS2 more efficiently. Once inside the cells, the virus takes over the translation machinery effectively by three mechanisms. At the same time, it starts to remodel the cells. Some infected cells fuse with neighboring cells to form syncytia, which is not found in the SARS-CoV virus. The syncytia might live longer and produce more copies of the virus [10]. All these features result in the SARS-CoV-2 strain having high transmissibility and fatality.
Variants
Compared with DNA viruses, RNA viruses have higher mutation rates, ranging from 10-6 to 10-4 substitutions per nucleotide, per round of copying. After its outbreak, more than 4000 SARS-CoV-2 mutation have been detected. The viral variants are the product of mutations which come from transcription or translation errors during viral replication [11]. “Some variants are variants of concern (VOCs), which refer to variants with an alteration in the S protein Receptor Binding Domain (RBD), which significantly improves the binding capability, leading them to have a high transmissibility, increased morbidity, or increased immune evasion”. In Figure 1 shows some variants and their clade, and all VOCs [11]. According to the WHO, previous circulating VOCs include Alpha, Beta, Gamma, Delta variants, and the Omicron variant is listed as the currently circulating VOC (access on June 19, 2022). Each of these 5 variants, at some point in time, have been related to a dramatic increase in COVID-19 cases among several nations at the same time.
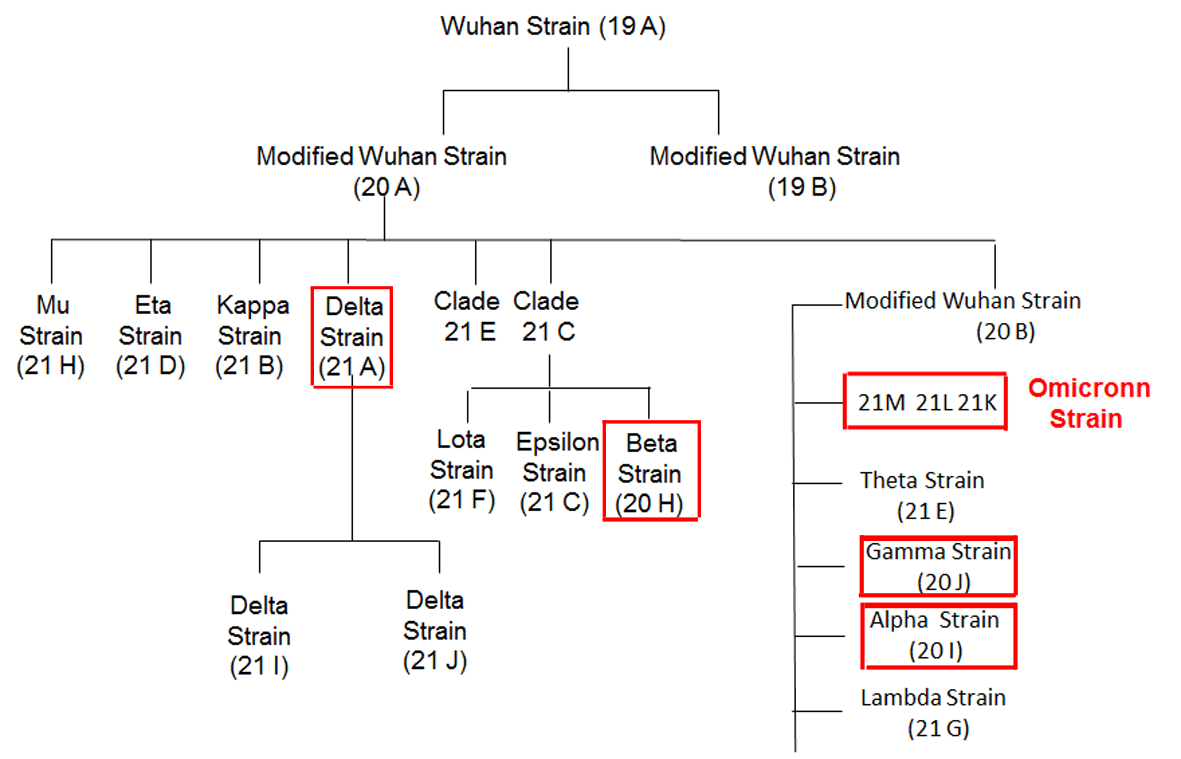
Figure 1: Variants of SARS-Cov-2, including all VOCs, which are in red rectangles, and their clade. This figure is modified from SARS-CoV-2 variants and vulnerability at the global level [11].
Omicron
Like any other virus, random mutations accumulate in SARSCoV- 2. S protein S1 subunit is the hot spot of mutation which can change the virus’s virulence, transmissibility, and immune evasion [12]. The Omicron variant was first detected in Gauteng province in South Africa in the middle of November 2021 [13]. On Nov 26, 2021, WHO designated this variant (B.1.1.529) a VOC [14]. Now, it is the dominant variant in all nations. It carries more than 60 alterations, deletions, and insertion mutations, a high percentage of them found in other VOCs, and at least 32 mutations in the S protein. It has 15 mutations in the RBD, some of them in viral replication proteins, like NSP12 and NSP14 [15-16]. The specific changes in the S protein (mutations in RBD, and N-terminal), make it more transmissible, even among vaccinated people15, as studies demonstrated that mutations in RBD are responsible for the escape from neutralized antibodies induced by vaccine [17]. The early double time for Omicron was 1.2 days, and for Delta was 1.5 days. Now, it is clear that it is substantially more spreadable, and the infection rates in Omicron were four time higher than that of the wild type, and the better interaction between the ACE2 receptor and S protein of the Omicron variant is the reason that Omicron has a higher infection rate than other VOCs. For the virulence of this variant, Omicron infection has milder symptoms and much less severe cases. The risk of hospitalization is less than that of the Delta variant. Vaccination, especial the booster, can significantly reduce the rate of being hospitalized and the rate of fatality [15].
The Impact of Covid-19 on Adolescent Mental Health
Since the start of pandemic, significant effort has been exerted to contain the spread of the virus. Isolation, quarantine, and even lockdown of huge cities like Shanghai all impact the mental health of the whole population. Quarantines and lockdowns are states of isolation that are psychologically painful and unpleasant for anyone who experiences them. Adolescents, who are at higher risk of developing mental health problems than adults, may be more vulnerable to the adverse effects of isolation [18]. They could not accurately identify the veracity of information about the COVID-19 pandemic due to the rapid flood of complex information on the Internet, and they had to study online at home as their schools had been closed. Thus, they may easily develop feelings of loss of control, negative emotions and behaviors, and their relationship with their parents may also be affected [19-20]. The repercussions of COVID-19 on adolescents’ mental health are mainly manifested in three aspects: emotion, behavior, and parent-child relationship. First, since the outbreak of the pandemic, the incidence of emotional problems in adolescents has increased. For example, in one study, researchers have shown that changes in adolescents’ emotional conditions were mentioned by 85.7% of the parents, manifested as boredom, worry, irritability and nervousness [21].
In another study, scholars have reported that Wuhan adolescents’ anxiety symptoms were significantly higher than in other urban areas during the epidemic [22]. Other studies have shown a feeling of isolation, apathy, and increased irritability among adolescents [19,23]. Moreover, there is also research suggesting that COVID-19 might influence adolescents’ adjustment in a cascading fashion, and adolescents whose parents are infected, served as first-line medical staff, or died due to COVID-19 might experience more severe mental health impacts than other adolescents [22]. Second, negative emotions can also result in greater irritability, aggressiveness and oppositional behaviors among adolescents [19]. The most frequent symptoms were regressive behaviors, oppositional behaviors, loss of appetite, and inattention [21,24]. During the lockdown, most parents also reported a change in their children’s behavioral condition. The changes reported were behavioral problems (reported by 44.2% of parents), sadness (reported by 43.7% of parents) and laziness (reported by 44.3% of parents) [25]. Third, home isolation dramatically increases the amount of time parents spend with their children and changes the parent-child relationship. Compared with non-COVID-19, 31.4% of families reported an increase in parent-child conflict in the last month.
In the context of COVID-19, parents are faced with greater financial pressure, which might lead to bad temper and an overreliance on less effective parenting approaches. Researchers found that Wuhan adolescents’ parents were less warm and supportive and showed more emotional rejection toward their children compared to other urban areas during the Wuhan epidemic [22]. As a result, the relationship between parents and children may be strained by the outbreak. In addition, the shift from offline to online, whether at work or at school, has significantly increased the amount of time parents and children spend on electronic devices, which has also led to more parent-child conflicts.
Conclusion
Currently, huge numbers of people are still infected every day, including those who are vaccinated. However, most of them display mild symptoms, and the number of related hospitalizations and deaths every week is relatively low (2140 deaths last week in the US). In most countries, like China, India, and America, which have large populations, most people are vaccinated, and are receiving the booster. The impact of pandemic on the economy is decreasing. On the other side, the emergence of new variants of SARS-Cov-2 is continuing. With intensive research still ongoing, the development of more effective vaccines, and the cooperation of the whole world, we will ultimately win the war against the virus.
Acknowledgment
The authors would like to give thanks for the financial support and the editorial help of the Biomedical Journal of Scientific & Technical Research (BJSTR) for the publication of this paper. We also thank Shiyuan Huang of Cornell University for her help in the preparation of the manuscript.
Conflict of Interest Statement
The author declares no conflicts of interest.
References
- Kim Daniel (2022) Minimizing Public Health Consequences of the COVID-19 Pandemic: Let's Consider the Threat of a Triple Recession. Lancet Reg Health Am 8: 100176.
- Weiss SR, Leibowitz JL (2011) Coronavirus pathogenesis. Adv Virus Res 81: 85-164.
- Greenberg SB (2016) Update on human rhinovirus and coronavirus infections. Semin Respir Crit Care Med 37(4): 555-571.
- Yang Y, Peng F, Wang R, Yange M, Guan K, et al. (2020) The deadly coronaviruses: The 2003 SARS pandemic and the 2020 novel coronavirus epidemic in China. J Autoimmun 109: 102434.
- (2019) World Health Organization. MERS situation update.
- Sabir JS, Lam TT, Ahmed MM, Li L, Shen Y, et al. (2016) Co-circulation of three camel coronavirus species and recombination of MERS-CoVs in Saudi Arabia. Science 351: 81-84.
- Abdelrahman Z, Li M, Wang X (2020) Comparative Review of SARS-CoV-2, SARS-CoV, MERS-CoV, and Influenza A Respiratory Viruses. Front Immunol 11: 552909.
- Zhang YZ, Holmes EC (2020) A genomic perspective on the origin and emergence of SARS-CoV-2. Cell 181(2): 223-227.
- Zhou P, Yang XL, Wang XG, Hu B, Zhang L, et al. (2000) A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 579(7798): 270-273.
- Scudellari M (2021) How the coronavirus infects cells - and why Delta is so dangerous. Nature 595(7869): 640-644.
- Chavda VP, Patel AB, Vaghasiya DD (2022) SARS-CoV-2 variants and vulnerability at the global level. J Med Virol 94(7): 2986-3005.
- Das S, Samantha S, Banerjee J, Pal A, Giri, et al. (2022) Is Omicron the end of pandemic or start of a new innings? Travel Med Infect Dis 48:102332.
- Omicron variant: what you need to know | CDC.
- Technical Advisory Group on Virus Evolution. Update on Omicron.
- Islam F, Dhawan M, Nafady MH, Emran TB, Mitra S, et al. (2022) Understanding the Omicron variant (B.1.1.529) of SARS-CoV-2: Mutational impacts, concerns, and the possible solutions. Ann Med Surg (Lond) 78: 103737
- He X, Hong W, Pan X, Lu G, Wei X (2021) SARS-CoV-2 Omicron variant: Characteristics and prevention. MedComm 2(4): 838-845
- Garcia-Beltran WF, St Denis KJ, Hoelzemer A, Lam EC, Adam D Nitido, et al. (2022) mRNA-based COVID-19 vaccine boosters induce neutralizing immunity against SARS-CoV-2 Omicron variant. Cell 185(3): 457-466.
- Panchal U, Salazar de Pablo G, Franco M, Moreno C, Parellada M, et al. (2021) The impact of COVID-19 lockdown on child and adolescent mental health: systematic review. European Child & Adolescent Psychiatry 18: 1-27.
- Bera L, Souchon M, Ladsous A, Colin V, Lopez-Castroman J (2022) Emotional and Behavioral Impact of the COVID-19 Epidemic in Adolescents. Current Psychiatry Reports 24(1): 37-46.
- Huang Y, Huang J, Wang T, Xu S, Li J (2021) The Impact of the Corona Virus Disease 2019 Pandemic on Chinese Middle School Students' Self-Perceived Emotional States: A Wuhan Perspective. Frontiers in Psychology 12: 740879.
- Orgiles M, Morales A, Delvecchio E, Mazzeschi C, Espada J P (2020) Immediate Psychological Effects of the COVID-19 Quarantine in Youth from Italy and Spain. Frontiers in Psychology 11: 579038.
- Chen S, Cheng Z, Wu J (2020) Risk factors for adolescents' mental health during the COVID-19 pandemic: a comparison between Wuhan and other urban areas in China. Globalization and Health 16(1): 96.
- Waite P, Pearcey S, Shum A, Raw J A L, Patalay P, et al. (2021) How did the mental health symptoms of children and adolescents change over early lockdown during the COVID-19 pandemic in the UK? JCPP advances 1(1): e12009.
- Pisano L, Galimi D, Cerniglia L (2020) A qualitative report on exploratory data on the possible emotional/behavioral correlates of Covid-19 lockdown in 4-10 years children in Italy.
- Stassart C, Wagener A, Etienne A M (2021) Parents' Perceived Impact of the Societal Lockdown of COVID-19 on Family Well-Being and on the Emotional and Behavioral State of Walloon Belgian Children Aged 4 to 13 Years: An Exploratory Study. Psychologica Belgica 61(1): 186-199.
