Research Article
Assessment of Dentists’ Knowledge Concerning the
Management of Breastfeeding Patients in Dental Office
Aranka Ilea1, Adela Cristina Lazăr1, Adriana Emanuela Morar2, Adina Bianca Boșca*3, Dan Buhățel1,
Anca Ionel1, Claudia Nicoleta Feurdean1, Anida Maria Băbțan1, Nausica Bianca Petrescu1, Ioana
Codruța Mirică1, Willi Andrei Uriciuc1, Roxana Ioana Bordea1, Arin Sava1, Radu Septimiu Câmpian1
and Alina Simona Șovrea3
Author Affiliations
1Department of Oral Rehabilitation, Oral Health and Dental Office Management, “Iuliu Hațieganu” University of Medicine and Pharmacy
Cluj-Napoca, Romania
2Postgraduate student of Faculty of Dentistry, “Iuliu Hațieganu” University of Medicine and Pharmacy Cluj-Napoca, Romania
3Department of Histology, Faculty of Medicine, “Iuliu Hațieganu” University of Medicine and Pharmacy Cluj-Napoca, Romania
Received: March 01, 2019 | Published: March 08, 2019
Corresponding author: Bianca Adina Boșca, Department of Histology, Faculty of Medicine, “Iuliu Hațieganu” University of
Medicine and Pharmacy Cluj-Napoca, Romania
DOI: 10.26717/BJSTR.2019.15.002736
Also View In:
Introduction: Breastfeeding is the feeding of babies and young children with milk
from a woman’s breast. Breastfeeding has numerous health benefits, including the lower
risk for respiratory tract infections, asthma, diarrhea, food allergies, type 1 diabetes, and
leukemia. It may also improve cognitive development and prevent obesity in adulthood.
Purpose: To assess the dentists’ medical knowledge regarding the dental treatment
allowed during the breastfeeding period.
Methodology: In this study were included active dentists. An online questionnaire
was applied. The questionnaire was anonymous and the responses were collected online.
The questions assessed the therapeutic approach of the patients during the breastfeeding
period, what kind of treatments they perform in this category of patients and the time
chosen for the dental treatments. The last category of questions collected data about the
medication used or prescribed in breastfeeding patients. The data was analyzed using the
descriptive statistics and the results were presented as means.
Results: More than half of the doctors surveyed would treat a breastfeeding woman
in any emergency situations, only if she postpone breastfeeding for the next 24 hours.
About 85% of the respondents will perform the anesthesia in a nursing woman, but about
just 1/3 will use mepivacaine and less than 3% will use lidocaine, anesthetic substances
admitted in a breastfeeding woman. In our study, about 90% of doctors who indicated the
administration of an antibiotic to a breastfeeding woman chose a synthetic penicillins drug
that are admitted during the lactation period.
Conclusion: Most dentists have insufficient knowledge regarding the treatments that
can be performed in breastfeeding women. Therefore, post-graduate courses are required
to update the knowledge of dentists in this domain.
Keywords: Breastfeeding; Nursing;
Infant; Dental Treatment; Dentistry;
Dental Procedures
Breastfeeding, also known as nursing, is the feeding of babies and young children with milk from a woman’s breast
[1]. Health professionals recommend that breastfeeding begin within the first hour of a baby’s life and continue as often
and as much as the baby wants [2,3]. During the first few weeks of
life babies can be nursed roughly every two to three hours and the
duration of a feeding is usually ten to fifteen minutes on each breast
[4]. Older children can be breastfed less often [5]. Mothers may
express their milk using breast pumps, so that it can be used later when breastfeeding is not possible [1]. Breastfeeding has a number
of benefits to both mother and baby, that infant formula lacks [3,6].
Deaths of an estimated 820,000 children under the age of five could
be prevented globally every year by increasing breastfeeding [7].
Breastfeeding decreases the risk of respiratory tract infections and
diarrhoea, both in developing and developed countries [2,3]. Other
benefits include lower risks of asthma, food allergies, type 1 diabetes, and leukemia [3]. Breastfeeding may also improve cognitive
development and prevent obesity in adulthood [2]. Mothers may
feel pressured to breastfeed, but in the developed world, children
generally can grow up normally when are bottle fed [8].
Benefits for the mother include: less blood loss following
delivery, better uterus shrinkage, and decreased postpartum
depression [3]. Breastfeeding delays the return of menstruation
and fertility, a phenomenon known as lactational amenorrhea
[3]. Long term benefits for the mother include decreased risk of
breast cancer, cardiovascular disease, and rheumatoid arthritis
[3,7]. Moreover, breastfeeding is less expensive than infant
formula [9,10]. Health organizations, including the World Health
Organization (WHO), recommend breastfeeding exclusively in the
first six months [2,3,11]. This means that no other foods or drinks
other than possibly vitamin D are typically given [11]. After the
introduction of solid foods at six months of age, recommendations
include continued breastfeeding until one to two years of age or
more [2,3]. Globally about 38% of infants are only breastfed during
their first six months of life [2]. In the United States in 2015, 83%
of women begin breastfeeding and 58% were still breastfeeding at
6 months, although only 25% exclusively [12]. Medical conditions
that contraindicate breastfeeding are rare [3]. Mothers who take
certain recreational drugs and medications should not breastfeed
(e.g. - antiretroviral medications, chemotherapy agents, sleep-aid
medicine, lithium and lamotrigine) [13]. Smoking, limited amounts
of alcohol, or coffee are not reasons to avoid breastfeeding [14-16].
To assess the dentists’ knowledge regarding the dental
treatments that can be performed in breastfeeding women and how
to prescribe drugs for these patients in the dental office.
An online questionnaire regarding the management of
breastfeeding patients in the dental office was administered
through the www.isondaje.ro platform such as was described by
Ilea et. al [17]. The study was attended by 128 dentists, of various
specialties, aged between 25 and 55 years. The questionnaire
was anonymous and the responses were collected online. The
first category of questions assessed the therapeutic approach of
the breastfeeding patients, what kind of treatments they perform
in this category of patients and the time chosen for the dental
treatments. The questions about the dental treatments, endodontic
treatment for pulp pathology, specific treatment for gingivitis and
chronic periodontitis, and the dental extractions performed in a
breastfeeding patient had five variants of response:
a) In emergency cases only
b) After the breastfeeding period ceased
c) I would perform such treatment at any time, but without
anesthesia
d) I would perform the treatments at any time, and if
anesthesia is necessary, I recommend the expression and the
discarding of the next milk
e) I perform dental treatments at any time and if anesthesia
is required, I choose an anesthetic that is compatible with
breastfeeding
The second category of questions evaluated the doctors’
recommendation to perform dental x-rays in breastfeeding
patients. The last category of questions evaluated the medication
used or prescribed for breastfeeding patients. When asked about
the use of anesthetic substances in a breastfeeding woman, there
were only two variants of response: I do not perform anesthesia
in a breastfeeding woman, or yes, I do the anesthesia, followed
by an open response to be completed the most commonly used
anesthetic. Data were analyzed using Microsoft Excel and the
results were exemplified using descriptive statistics.
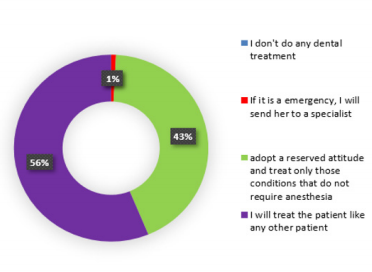
The Attitude of Dentists Regarding Treatments that Can
Be Performed in a Breastfeeding Patient
The question referring to the attitude adopted at the time of the
anamnesis when they are informed that the patient in the dental
chair is breastfeeding, had four variants of response:
b) If it is an emergency, I send her to the specialized hospital
service;
c) I have a reserved attitude and treat only those conditions
that do not require anesthesia;
d) I treat a breastfeeding woman like any other patient. Of
the total of 128 subjects, no dentist chose not to treat a nursing
patient
e) one dentist (1%) chose the second option
f) 55 doctors (43%) chose the third option
g) and 72 subjects (56%) chose to treat a pregnant woman
like any other patient
h) It can be seen that the last answer was chosen by more
than half of the subjects (Figure 1).
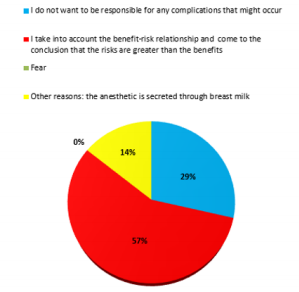
The Reasons Why a Dentist Would Not Treat a Patient
Who is Breastfeeding
The next question in the questionnaire was addressed only to
subjects who chose not to treat a breast-fed patient or had reserved
attitude, which was one of the first three variants of the previous
question:
a) I do not perform any dental treatment,
b) If it is an emergency, I send her to the hospital specialty
service or
c) I have a reserved attitude and treat only those conditions
that do not require anesthesia.
There were four possible answers to the question “What are the
reasons why you do not treat a nursing patient?”:
a) I do not want to be responsible if some complications
arise;
b) I take into account the benefit-risk ratio and if the risks
are greater than the benefits, I do not perform any treatment;
c) fear; and
d) other reasons (open-ended variation). Only seven
responses were collected. Two doctors (29%) chose the first
response
e) four doctors (57%) chose the second variant
f) none of the doctors chose the fear, as a reason of not
treating a breastfeeding patient, and one doctor (14%) selected
the last option
g) and responded that the reason for not treating a nursing
patient was that the anesthetic is excreted in breast milk (Figure
2).
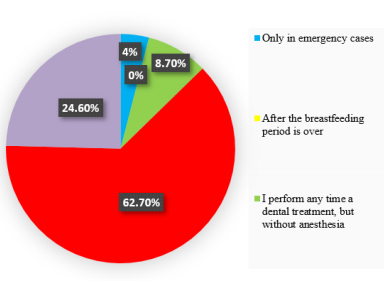
Dental Treatments in a Breastfeeding Patient
When asking about the dental treatments performed in a
breastfeeding patient, there were 128 responses, out of which 5
responses (4%) were the first variant
a) There was no response for the second option
b) 11 responses (8.7%) were the third option
c) 79 responses (62.7%) were the fourth option
d) and 31 responses (24.6%) were the last option
e) Therefore, most dentists would perform dental
treatments at any time, but would recommend to the patient
not to breastfeed after the anesthesia and to discard the next
milk. About a quarter of the respondents would choose an
anesthetic compatible with breastfeeding (Figure 3).
Endodontic Treatments in a Nursing Patient
When asking about the endodontic treatment (for pulpitis or
pulp necrosis) in a breastfeeding patient, there were 128 responses,
out of which 6 responses (4.8%) were the first variant
a) 1 response (0.8%) was the second variant
b) 7 responses (5.6%) were the third option
c) 82 responses (65%) were the fourth variant
d) and 30 responses (23.8%) were the last variant
e) Most doctors would perform an endodontic treatment
at any time but would recommend to the patient that after the
anesthesia they should express milk and discard it. Almost a
quarter of the respondents would choose an anesthetic that is
compatible with breastfeeding.
Specific Treatment for Gingivitis in a Breastfeeding
Patient
The question about the specific treatment for gingivitis in a
breastfeeding patient had a total of 128 responses, out of which six
answers (4.7%) were the first variant
a) two answers (1.6%) were the second option
b) 20 answers (15.9%) were the third variant
c) 64 answers (50.8%) were the fourth variant
d) and 34 answers (27%) were the last variant
e) Half of physicians would perform the specific treatment
for gingivitis at any time but would recommend the discard
of the milk after the anaesthesia. More than a quarter of the
respondents would choose an anaesthetic that is compatible
with breastfeeding.
Specific Treatment for Chronic Periodontitis in a Nursing
Patient
The question about the periodontal treatment in a breastfeeding
patient, had a total of 128 responses, of which 6 responses (4.8%)
were the first variant
a) one response (0.8%) was the second variant
b) 11 responses (8.6%) were the third variant
c) 75 responses (58.6%) were the fourth variant
d) and 35 responses (27.2%) were the last variant. More
than half physicians would perform periodontal treatment at
any time, but would recommend the expression and discarding
of the next milk. More than a quarter of the respondents would
choose an anesthetic that is compatible with breastfeeding.
Dental Extractions in Breastfeeding Patients
When asking about the dental extraction performed in a
breastfeeding patient, there were 128 answers, out of which 17
answers (13.3%) were the first variant
a) 5 responses (3.9%) were the second variant
b) none of the doctors chose the variant
c) 77 responses (55.5%) were the fourth variant
d) and 35 responses (27.3%) were the last variant
e) More than half physicians would perform an extraction
at any time but would recommend that the patient should
express and discard the next milk. More than a quarter of the
respondents would choose an anesthetic that is compatible
with breastfeeding (Figure 4).
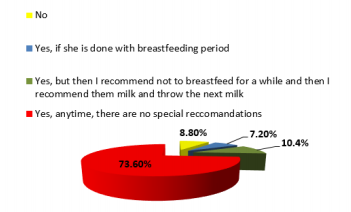
Performing Dental X-Rays in a Breastfeeding Patient
When asked about recommending dental x-rays in a
breastfeeding patient, there were four variants of answer:
a) No;
b) Yes, if she passed the breastfeeding period;
c) Yes, but then I recommend not to breastfeed for a while
and then express and discard the next milk;
d) Yes, anytime, without special recommendations. Of the
total of 125 responses, 11 responses (8.8%) were the first
variant
e) 9 responses (7.2%) were the second variant
f) 13 responses (10.4%) were the third variant
g) and 92 responses (73.6%) were the last variant (Figure 5). The answer to this question showed that regarding to dental
radiographs in a nursing patient, about ¾ of the doctors were
well informed.
Use of Anesthetics in a Breastfeeding Patient
The question about the use of anesthetic substances in a
breastfeeding woman had two variants of response:
a) I do not perform anesthesia in a breastfeeding woman;
and
b) Yes, I perform the anesthesia, which was followed by an
open question regarding the most commonly used anesthetic.
Of the 128 responses, 19 responses (14.8%) were the first
variant
c) 109 responses (85.2%) were the second variant
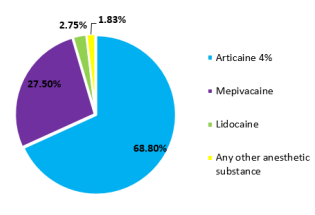
d) In the second variant, to the open question regarding the
anesthetic substances used, the 109 responses were divided as
follows: articaine 4% solution (68.8%), mepivacaine (27.5%),
lidocaine (2.75%) and any anesthetics (1.83%) (Figure 6). Most
of the respondents will perform the anesthesia in a nursing
woman, but about just 1/3 will use mepivacaine and less than
3% will use lidocaine, anesthetic substances admitted in a
breastfeeding woman.
Prescription of Antibiotics in a Breastfeeding Patient
The question about prescribing antibiotics to a breastfeeding
patient had two variants of response:
a) No and
b) Yes, which was followed by an open question regarding
the most frequently prescribed antibiotic. Out of the 128
answers, 74 answers (57.8%) were the first variant
c) and 54 answers (42.2%) were the second variant
d) Regarding the most frequently prescribed antibiotics,
the 54 responses were divided as follows: amoxicillinclavulanic acid (48%), amoxicillin (31%), ampicillin (7%),
cefuroxime (3.6%), other cephalosporins (1.8%), clindamycin
(1.8%), prescribed only after consulting the pediatrician or
neonatologist (5%), prescribing only after consulting the
gynecologist (1.8%). Almost half of the doctors would prescribe
the same type of antibiotic which they usually prescribe in
the dental office. About 90% of doctors who indicated the
administration of an antibiotic to a breastfeeding woman
chose a synthetic penicillins drug that are admitted during the
lactation period.
The hormonal changes associated with breastfeeding were
discussed with reference to the findings from animal studies. Both
lactation and stimulation of breastfeeding are phenomena involving
hormones in the anterior and posterior lobe of the pituitary gland.
In women and animals, complex hormonal changes occur during
pregnancy, being represented by the estrogen and progesterone,
reaching peak levels towards the end of pregnancy. The most
important postpartum hormone is prolactin, which initiates
lactation. And the decrease in estrogen and progesterone levels,
once the fetus and the placenta are delivered, helps to stimulate
lactation [18]. An indirect effect of the high levels of prolactin,
which supports breastfeeding, is the increased need for calcium in
the nursing woman. Some authors stated that during breastfeeding,
300-400 mg of calcium are transferred to breast milk, while other
authors have stated that during lactation, calcium is preserved by
the kidney to maintain the bone metabolism. Bone calcium loss is
counterbalanced by higher levels of vitamin D, growth hormone
changes, prolactin, and also by nutritional habits and lifestyle
[19,20]. After birth, the patient is in a recovery period, called period
of lice. This physiological period lasts about six to eight weeks and
is necessary for the body to be restored after birth.
In our study, referring to the dental treatments, most dentists
would perform it at any time, but would recommend to the patient
not to breastfeed and express and discard the next milk after the
anesthesia. The main and most important issue raised in the dental
office is the administration of drugs. In our study, almost half
of the doctors would prescribe the same type of medicine which
they usually prescribe in the dental office, probably based on their
knowledge regarding the properties of the drug. The prescription
of medication during breastfeeding is a challenge for both the
patient and the physician. Therefore, many mothers are advised to
express and discard the breast milk if they take certain medication. However, this advice is often based on limited medical information.
Some studies reviewed the evidence on certain medicines that are
safe or others that should be avoided during breastfeeding. Dentists
should be familiarized with the risks and benefits of prescribing
for a nursing patient certain classes of drugs: antibiotics, local
anesthetics, and emergency medications [21].
The milk secretion occurs 24-48 hours after birth. Most substances
or drugs ingested by the mother are secreted into the breast milk.
Antibiotics can be ingested by the baby through breast milk if the
mother is under antibiotic treatment for a variable period of 5 - 7
- 10 days required as adjuvant treatment of oral cavity pathology.
This results in early exposure of the infant to antibiotics, which
will reduce the long-term breastfeeding beneficial effects (such as
reducing the frequency of infections and the risk of overweight)
and also, the infant’s microbiota can be modified [22]. In our
study, about 90% of doctors who indicated the administration
of an antibiotic to a nursing woman chose a synthetic penicillins
drug that are admitted during the lactation period. Almost half
of them indicated the administration of amoxicillin-clavulanic
acid. Although the concentration of this antibiotic is low in breast
milk in order to produce infant toxicity (0.68-1.3 μg / ml when
administering 1g of amoxicillin - clavulanic acid), there is the
possibility of hypersensitization of the infant to this drug and the
alteration of the intestinal microbiota, so this should be avoided
[23].
Some authors recommend that after dental treatments that
require the loco-regional anesthesia, the baby’s first suckling
should be suppressed, and milk be expressed and discarded [24].
In our study, most dentists would perform a dental treatment at
any time but would recommend to the patient not to breastfeed
after the anesthesia. It is important to know how the drugs are
secreted into the breast milk and what factors are involved, in
order to know what drugs can be safely administered. According
to the literature, the use of lidocaine, mepivacaine, and bupivacaine
for local anesthesia is considered compatible with breastfeeding
because of low levels in breast milk. Thus, the relative infant dose
(RID), which is calculated by dividing the infant’s dose via milk by
the mother’s dose, is 0.5-3.1 for lidocaine and 0.9 for bupivacaine.
In our study, approximately two-thirds of physicians indicated local
anesthesia with articaine and only about 1/3 with mepivacaine,
which showed insufficient knowledge among respondents [25].
Multiple situations requiring pharmacological treatment may occur
in breastfeeding women. Due to the many health benefits of breast
milk in infants, breastfeeding should only be discontinued when
the drug necessary for the mother could be harmful to the child.
There is no reliable evidence that most drugs cause adverse effects
to the breastfed child. Moreover, interruption of breastfeeding,
even temporary, may be difficult. Therefore, decisions on the
use of medication should be based on correct information. Most
antibiotics are considered compatible with breastfeeding [26].
There is insufficient knowledge of an appreciable number
of dentists in related to the treatments that can be performed
in breastfeeding women. Therefore, postgraduate courses and
continuous medical education would be required in order to update
the knowledge of dental practitioners.
Aranka Ilea, Adela Cristina Lazăr and Adriana Emanuela Morar
have equals contributions as first authors of the article.
- Andreas NJ, Kampmann B, Mehring Le Doare (2015) Human breast milk:
A review on its composition and bioactivity. Early Hum Dev 91: 629-635.
- Martin CR, Ling PR, Blackburn GL (2016) Review of Infant Feeding: Key
Features of Breast Milk and Infant Formula. Nutrients 8(5): 279.
- Bagga N, Nadipineni R, Mohamed A, Poddutoor P, Chirla DK (2018) A
quality initiative to improve exclusive breast milk feeding in preterm
neonates. Int J Pediatr Adolesc Med 5(4): 131-134.
- Ingram J, Johnson D, Copeland M, Churchill C, Taylor H (2015)
The development of a new breastfeeding assessment tool and the
relationship with breastfeeding self-efficacy. Midwifery 31(1): 132-137.
- Ip S, Chung M, Raman G, Trikalinos TA, Lau J (2009) A summary of
the agency for healthcare research and quality’s evidence report on
breastfeeding in developed countries. Breastfeeding Med 4(1): 17-30.
- Victora CG, Bahl R, Barros AJ, França GV, Horton S, et al. (2016)
Lancet Breastfeeding Series Group. Breastfeeding in the 21st century:
epidemiology, mechanisms, and lifelong effect. Lancet 387(10017): 475-
490.
- Lawrence RA, Lawrence RM (2011) Breastfeeding: A Guide for the
Medical Profession. Elsevier Health Sciences. 2011, The (7th edn). Mosby,
an imprint of Elsevier Inc, pp. 227-228.
- Ballard O, Morrow AL (2013) Human Milk Composition: Nutrients and
Bioactive Factors. Pediatr Clin North Am 60(1): 49-74.
- (1997) Breastfeeding and the use of human milk. Pediatrics 100(6):
1035-1039.
- Bzikowska Jura A, Czerwonogrodzka Senczyna A, Oledzka G, Szostak
Wegierek D, Weker H, et al. (2018) Maternal Nutrition and Body
Composition During Breastfeeding: Association with Human Milk
Composition. Nutrients 10(1379): 1-15.
- Kramer MS, Kakuma R (2012) Optimal duration of exclusive
breastfeeding. The Cochrane Database of Systematic Reviews 8(8):
CD003517.
- (2018) Results: Breastfeeding Rates. Center for Disease Control and
Prevention (CDC).
- (2013) Are there any special conditions or situations in which I should
not breastfeed? National Institutes of Health.
- May PA, Hasken JM, Blankenship J, Marais AS, Joubert B, et al. (2016)
Breastfeeding and maternal alcohol abuse: prevalence and effects on
child outcomes and fetal alcohol spectrum disorders. Reprod Toxicol 63:
13-21.
- Wright MJ, Bentley ME, Mendez MA, Adair LS (2015) The interactive
association of dietary diversity scores and breast-feeding status with
weight and length in Filipino infants aged 6-24 months. Public Health
Nutr 18(10): 1762-1773.
- Chamberlain C, OMara Eves A, Oliver S, Caird JR, Perlen SM, et al. (2013)
Psychosocial interventions for supporting women to stop smoking in
pregnancy. Cochrane Database Syst Rev 23(10): CD001055.
- Ilea A, Lazăr AC, Morar AE, Boșca AB, Băbțan AM, et al. (2019) Assessment
of Dentists’ Knowledge Concerning the Management of Pregnant Women
in the Dental Office. Biomed J Sci & Tech Res 15(2): 1-9.
- Voogt J (1978) Control of hormone release during lactation. Clin Obstet
Gynaecol 5(2): 435-455.
- Kovacs CS (2001) Calcium and bone metabolism in pregnancy and
lactation. J Clin Endocrinol Metab 86(6): 2344-2348.
- Kalkwarf HJ (1999) Hormonal and dietary regulation of changes in bone
density during lactation and after weaning in women. J Mammary Gland
Biol Neoplasia 4(3): 319-329.
- Hotham N, Hotham E (2015) Drugs in breastfeeding. Australian
Prescriber 38(5): 156-159.
- Korpela K, Salonen A, Virta LJ, Kekkonen RA, De Vos WM (2016)
Association of Early-Life Antibiotic Use and Protective Effects of
Breastfeeding: Role of the Intestinal Microbiota. JAMA Pediatr 170(8):
750-757.
- De Sá Del Fiol F, Barberato Filho S, de Cássia Bergamaschi C, Lopes LC,
Gauthier TP (2016) Antibiotics and Breastfeeding. Chemotherapy 61(3):
134-143.
- Donaldson M, Goodchild J (2012) Pregnancy, breast-feeding and drugs
used in dentistry. Am J Dent Assoc 143(8): 858-871.
- Smathers AB, Collins S, Hewer I (2016) Perianesthetic Considerations
for the Breastfeeding Mother. J Perianesth Nurs 31(4): 317-329.
- Bar Oz B, Bulkowstein M, Benyamini L, Greenberg R, Soriano I, et al.
(2003) Use of antibiotic and analgesic drugs during lactation. Drug
Safety 26(13): 925-935.
 Research Article
Research Article