 Research Article
Research ArticleAbstract
Appendicitis is an inflammation of the appendix causes pain in lower right abdomen; it is affects approximately 10% of the world population. The role of parasitic infection in an etiology of acute appendicitis has been discussed for more than 100 years. The current study aims to evaluate the prevalence of parasitic infection in surgically removed appendices from patients in Al-Jalla – hospital Benghazi, Libya. A retrospective study included patients who had acute appendicitis during January to November 2012. One hundred and seventy-five surgically removed appendices were examined for the presence of parasitic infections. Parasites were found in 120 cases (68.6%). Entamoeba histolytica was the most frequently encountered parasite 61 (50.8%) followed by Blastocystis hominis 45 (37.5%) and Entamoeba coli 42 (35%). Giardia lamblia and Entrobius vermicularis were also found with rates 6 (5 %) and 8 (6.7 %) respectively. The results revealed that the most frequently operated people are of age between 10-19 with no significant differences between age groups (P=.138) No differences were found between gender in relation to appendicitis or the presence of parasites. The incidence rates of appendicitis and parasitic infections were high during the months of May, June, July, however the difference was not statistically significant. There was a significant difference between the presence of abnormal growth or stones and parasitic infection (P<0.025). It comes clear from our results that there is association between parasitic infection of the appendix and acute appendicitis.
Keywords: Intestinal parasites; Appendix; Libya; Acute appendicitis
Introduction
Human appendix is a finger-like pouch attached to the large intestine and located in the lower right area of the abdomen [1]. It is a hollow tube with mucous membrane, and a muscle similar to that of the caecum. It’s size and shape are quite variable, but generally about 9 cm long. It may turn up wards behind the caecum pointing out towards the groin-the retro-caecal position or it may lie on the front of the caecum immediately under the anterior abdominal wall [1]. The appendix does not function in digestion but like the tonsils, it contains numerous lymphatic nodules and its subject to inflammation a condition called appendicitis. This is commonly detected in its later stages by pain in the lower right quadrant of the abdomen. If the appendix ruptures, infectious material can spread throughout the surrounding body cavity, causing inflammation of the peritoneum (peritonitis). This dangerous event may be pre vented by surgical removal (appendectomy) of the inflamed appendix [1]. Appendicitis is caused by multifactorial reasons.
Fecal stasis and lymphoid hyperplasia are the most common causes of appendicitis whereas unusual causes of appendicitis are intestinal parasites and tumors. Parasites may sometime influence appendix. This situation can differ between an innocent reaction and an inflammatory response threatening life. A reported 250,000 appendectomies are performed annually with 15% result in removal of normal appendix. Around 4 -8% of the children are reported to be infected by parasite globally. Parasitic infections may cause symptoms mimicking acute appendicitis; however, their role in the causation of acute appendicitis remains speculative. Sporadic cases of appendicitis have been attributed to parasitic infections [2,3]. Parasitic infections are ubiquitous on a worldwide basis and are seen in high numbers in developing countries. The presence of parasite in the appendix may cause appendicecal colic even without eliciting acute inflammation. The presence of pin worm in the appendix has been shown to cause symptoms of appendicitis or appendicecal colic but frequently without any histological evidence of acute inflammation.
This colic due to parasitic infestation is explained by the hypothesis of appendicecal lumen obstruction [4]. The parasitic infestation is a leading cause of iron deficiency anemia, growth retardation, while heavy infestation with both round worm and whip worm causes protein energy malnutrition. Moreover, it can lead to intestinal obstruction in infested children [5]. Timely diagnosis and treatment with de-worming of the patients prevent probable future complications that may necessitate surgical procedure.
Material and Methods
Sampling site. This study was conducted in Benghazi city. The city of Benghazi is situated between degree of latitude (32°10’N) and longitude (20°06’E). It is the second largest city in Libya occupying an area of approximately 240 km2. It is situated on the eastern southern coast of Mediterranean Sea north-east of Libya. The population of the entire district was 670,797 in the 2006 census.
Collection of Samples
Samples were collected from Al jalla hospital. This hospital is located in center of Benghazi and it is one of the biggest hospitals in the city. It is the main hospital of the most surgical operations done in east region of Libya. One hundred and seventy-five removed appendices were collected after appendectomy during the period from January to November 2012. These specimens were preserved in 10 % formalin in clean tubes. All specimens were labeled with the patient age, gender and date of operation.
Parasitological Examination
Removed appendices were brought to the research laboratory in zoology Department for the process of examination, each appendix was opened longitudinally and placed in petri dish contains 0.85% saline solution. The contents were carefully examined under dissecting microscope for the presence of parasites and any foreign bodies. All encountered worms were counted, removed and preserved in 70% ethanol. Appendices contain stone or abnormal bodies were recorded as well. The contents of the appendices were also examined for micro -parasites (cyst- oocysts- eggs) by direct and indirect saline -iodine smears and formalin - ethyl acetate sedimentation technique then examined under microscope using low power (10x) and high-power objectives (40x,100x).
Statistical Analysis
Chi-square x2 was employed to find out the significance or non-significance of the relationships between age, gender, months and the presence or absence of the parasitic infections. Level of significant (p<0.025). t-test (p<0.025), also we used ANOVA with (p<0.05). All analysis was computed in windows environment of statistical of program (SPSS) version 17.
Results
The present results revealed that appendicitis is common disease in people living in Benghazi city and its surround areas sense there were about 18 appendectomy operation every month. The results showed that 120 (68.6%) with high significance (χ2 = 24.914a, df= 3, p=0.000) of the total removed appendices (n=175) were infected with parasites. Specifically, the following intestinal parasites were highly prevalent in patients with appendicitis., the most isolated parasite Entamoeba histolytica/E. dispar 61 (34.8% of 175 total removed appendices patients / 50.8 % of parasitic infected patients ), Blastocystis hominis45 (25.7 % of 175 total removed appendices / 37.5 % of parasitic infected ), Entamoeba coli 42 (24 % of 175 total removed appendices / 35 % of parasitic infected patients ), G.lamblia 6 (3.4% of 175 total removed appendices patients / 5 % of parasitic infected patients ), E. vermicularis 8 ( 4.5 % of 175 total removed appendices / 6.7 % of parasitic infected patients) (Table 1).
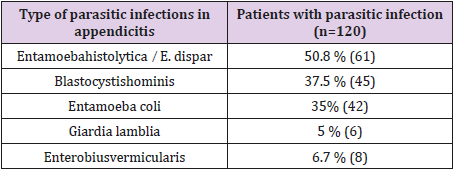
Table 1: Show different types of parasite isolated from patients with removed appendicitis their percentage (calculated from total infected with parasites number).
The highest prevalence of parasitic infection (75.9%) was recorded among individuals in the 10-19 years age category, followed by those of the 40-49- and 20-29-years age group (70.6%, 67.6 %) respectively. The lowest prevalence of parasitic infection (20.0 %) was observed among the individuals of age categories above 50 years as indicated in Table 2. Statistically, no significant difference was observed in the association between parasitic infection and age (X2 =6.958a, df=4, P=.138). The results presented in Table 3 shows the distribution of parasitic infections among gender (sex) in patients with appendicitis. 60(69.0%) females and 60(68.2%) males, indicating that both genders are equally susceptible to infection and the result showed no difference in the incidence of appendicitis between males and females (p=.821). Also there was no significant differences between the gender in relation to the presence of parasites.
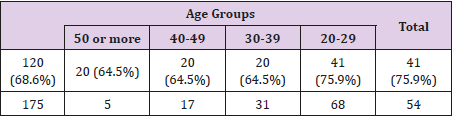
Table 2: The presence of parasites in removed appendices according to age groups.
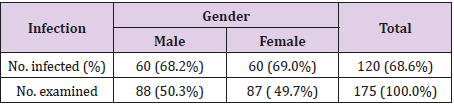
Table 3: Distribution of parasitic infections among gender (sex) in patients with appendicitis.
The results presented in Table 4 revealed that the peak incidence rate of appendicitis occurring during the months of May, June, July, 21.7%,27.4% and 21.7% respectively. Similar results also seen in relation to the presence of parasites in removed appendices. The rates were 17.1%, 20% and 16.6% in May, June, July respectively. Even that there were no significant differences between months and infection or disease (p>0.025). Out of the total removed appendicitis (175) twenty three appendices (13.1%) were found with abnormal growth and six (3.4%) were found with stones. In only one appendix (0.6%) there was stones and abnormal growth (Table 5). The results presented in Table 6 revealed that out of 23 abnormal growth appendices only five showed parasitic infection. On other hand five appendices were infected with parasites out of six showed presence of stones. And only one case with abnormal growth and stones was infected with parasites. There was a significant difference between the presence of abnormal growth or stones and incidence of parasitic infection. (p>0.025).
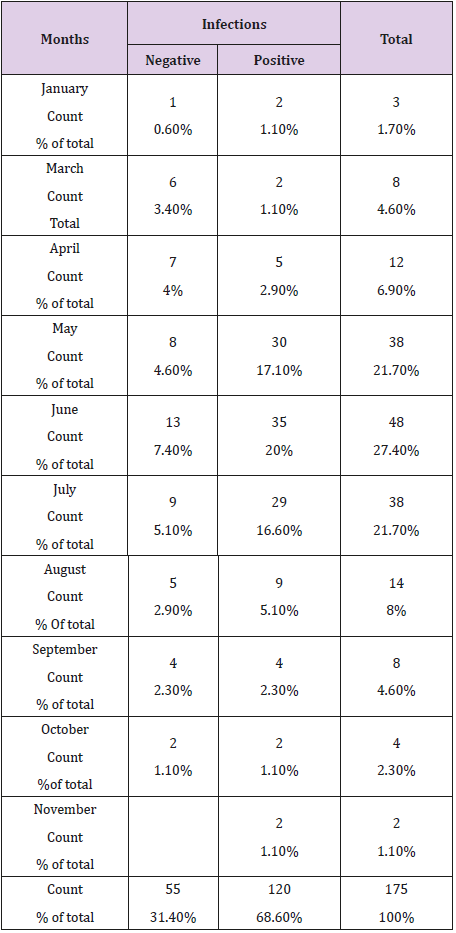
Table 4: Monthly incidence of appendicitis and the presence of parasites in the examined appendices.
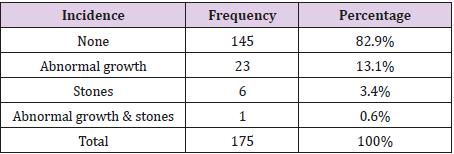
Table 5: The percentages of abnormal growth and stones incident in relation to the presence of parasites in removed appendices.
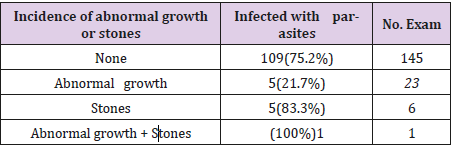
Table 6: The percentages of abnormal growth and stones incident in relation to the presence of parasites in removed appendices.
The distribution of intestinal parasites detected in patient with appendices. shown in Figure 1. Of the total study population 80 (45.7% of 175 total removed appendices/ 66.7% of parasitic infected harbored at least one parasite while intestinal parasites were found in 22.9 % (40 of 175 ) and 33.3% of parasitic infected were infected with two or more parasites of the removed appendices, the result show that the a high significant (p=0.00).
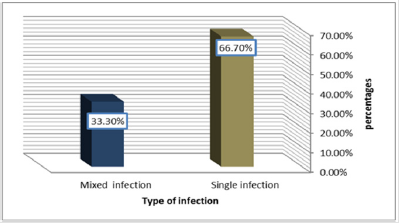
Figure 1: The percentages of single and mixed parasites recovered in the removed appendices. (n=120).
Discussion
Appendicitis is one of the most common disease all over the world. It affected approximately 7-10% of the world population [6- 8]. The present study indicates that appendicitis is a common disease in Benghazi city. One hundred and seventy-five appendectomy operation have been carried out in ten months. These results is consistent with other studies all over the world [6,9,10]. The author is not aware of any published records on the incidence of appendicitis in Libya. Generally the incidence of appendicitis varies substantially by country, geographical region, race, sex, age and seasons [9,11]. In third world the incidence of appendicitis is rare in the past and began to increase a century ago peaked about 1950 [12]. Changing to a Western lifestyle, including diets due to the increasing number of fast food restaurants where mainly highcarbohydrate low fiber diets and sweets could have contributed to the increase the incidence of appendicitis [13-16].The present study concentrated on the parasites (Protozoa, Cestoda, Trematoda and Nematoda ) of the appendix removed from different groups of patients in Al jalla–hospital.
This is a pioneering study the relationships of parasites to appendicitis. The predisposing factors to appendicitis are thought to be multifactorial including mechanical obstruction, inadequate dietary fiber, family susceptibility and viral, parasitic pathogens [17]. The association between parasitic infection of the appendix and acute appendicitis has been widely investigated [18-,20]. The results of this study have indicated that 68% of removed appendices were infected with parasites. This finding is in agreement with many authors [21-24]. these authors reported the hypothesis that the parasites can cause appendicitis. In contrast many other authors do not agree with this hypothesis [25,26]. In the present study three pathogenic parasites were recovered these are E. histolytica, E.vermicularis and G.lamblia. The same parasites reported in removed appendices from different parts of the world [3,24].The results also showed the presence of Blastocystis hominis in removed appendices. This parasites consider by many as nonpathogenic [27,28].
On other hand there are many reports indicate that this parasites is a pathogenic [29]. There is only one report in literature associated Blastocystishominis with appendicitis by Pasupati [30]. from Malaysia which consistent with the results of this study. So, the role of B. hominisin appendicitis should not overlook. The present study showed that about 4.5% of the total removed appendices were infested with E.vermicularis. It is one of the most common nematode parasites of human which flourish in the temperate zone where probably every child has been infected than once more in early childhood. The percentage of E. vermicularisin this study is slightly higher than incidence reported by [26,31]. On other hand results of this study is lower than those reported by others [25,32] from Egypt and Iraq respectively. In general, the rate of E. vermicularis in the appendices range from 0.2% up to 48% worldwide. The role of E. vermicularisin association to appendicitis is controversial [20,33,34].
Enterobius vermicularis is a common cause of appendicitis [23,31]. Its presence in the appendix can produce clinical feature of appendicitis “appendicitis colic “ resembling the disease [35]. Williams and Dixon (1988) suggesting that the eggs release from female pinworms may be a feature of appendiceal obstruction. On other hand many reports disagree with hypothesis of E. vermicularis involvement in appendicitis [18,35]. concluded that parasites in the appendix may produce symptoms which resemble acute appendicitis, but parasitic infection rarely causes acute appendicitis. E. histolytica is a second parasitic agent of acute appendicitis [18,25,32]. Acute appendicitis of amoebic origendoes not appear frequently [10]. In the present study 34.8% of removed appendices were infected with E .histolytica/dispar unfortunately no-attention has been made to separate the two species because of limited facilities. This result is in consistent with Okoliet al (2008) in south-eastern, Nigeria.
However, it is higher than those reported by other authors [25,32] were the rate of the E. histolytica/dispar ranges from 0.5% to 2.5% G.lambliais a common parasite of man , it has worldwide distribution, it was considered non pathogenic as it found in complete a symptomatic persons , However . There is now abundant evidence of pathogenic potential of Giardia [36]. The incidence rate of G. lambliain the present study 3.4% which is higher than incidence reported by Salihet [37] in Iraq. Other report in Iraq too by Abed-Al Rekabi [38] was higher than present study. Reviewing the literature no other reports on the association of G.lambliawith appendicitis . E. coli is a non-pathogenic parasite of human. The present study indicate that 24% of removed appendices were infested with this parasite which inconstant with the results reported by Pasupati [30]. Reviewing the literature no other reports on the association of E.coli with appendicitis.
The results of this study revealed that a higher percentage of patient who had parasites in their appendix fall within the 20-29 years old age group with 26% followed by age group 10-19 years and 30-40 years of age. This result in agreement with many reports [7,13]. Many researchers suggested that the age is a risk factor for both disease and parasitic infestation of appendix [3], while others denied the association [38]. The present study revealed that there was no significant difference between the incidence of appendicitis in males and females’ patients and also there was no difference in parasitic infestation in the appendices. This suggests that males and females are equally exposed to parasitic infection and gender may not necessarily be an important epidemiological determinant for appendicitis and parasites loads. This results in agreement the results reported by [34]. Other workers reported high incidence in males [7,17,24].
On other hand many authors found that females were more susceptible to disease [33]. These authors explained their results due to false diagnosis of appendicitis. The present study revealed that the highest incident of appendicitis and parasitic infestation occurred during summer months (May, June, July). similar results were reported by other authors [17,38]. The monthly variation may be explained by the increase of contaminated water and vegetable consumption during the hot weather.
Conclusion
This is pioneering study on the incidence of parasitic infection of appendices removed from patients in Al-jalla hospital, Benghazi city. Five intestinal parasites were recovered, namely Entamoebahistolytica, E. coli, G. lamblia, B.hominis and E. vermicularis. Sixty eight percent of examined appendices were infected with one or more parasites. The rate of these parasites will not be excluded , they may cause appendicitis or produce symptoms similar to that of appendicitis which may lead to false appendectomy. So, there is a need for treating the intestinal parasites before infecting the appendix. It will be worthwhile to continue the study of the prevalence and the causes of appendicitis in Libya which may give a comparative and comprehensive picture.
References
- Gillian P, Christopher RD (2006) Human Physiology: The Basis of Medicine, (3rd edition) Oxford University Press. London, UK, pp. 412-4 14.
- Karatepe O, Adag G, Tukenmez M, Battal M, Altiok M, et al. (2009) parasitic infestation as cause of acute appendicitis. Giornale Di Chivurgia 30(10): 426-428.
- Arca MJ, Gates RL, Groner JL, Hammond S, Caniano DA (2004) Clinical manifestations of appendiceal pinworms in children: an institutional experience and a review of the literature. Pediatric Surgery International 20 (5): 372-375.
- Yabanoglu H, Caliskan K, Aytac HO, Turk E,Karagulle E, Kayaselcuk F, et al. (2014) Unusualfindings in appendectomy specimens of adults: retrospective analyses of 1466 patients and a review of literature. Iran Red Crescent MedJ 16(2): e12931
- Ikramulah, Sarwar G, Aziz S, Khan MH (2009) Intestinal Worm Infestation in Primary School Children in Rural Peshawar. Gomal Journal of Medical Sciences 7(2): 132-136.
- Irvin TT (1989) Abdominal pain: a surgical audit of 1190 emergency admissions. British Journal of Surgery 76(11): 1121-1125.
- Engin O, Calik S, Calik B, Yildirim M, Coskum G (2010) Parasitic Appendicitis from past to present in Turkey. Iranian Journal of Parasitology 5(3): 57-63.
- Agresta F, Ansaloni L, Catena F, VerzaL A, Prando D (2014) Acute appendicitis: position paper,2013. World J Emerg Surg 9(1): 26.
- Jones BA, Demetriades D, Segal I, Burkitt DP (1985) The prevalence of appendiceal fecalthis in patients with and without appendicitis. A comparative study from Canada and South Africa. Annals of surgery 202(1): 80-82.
- Singh NG, Mannan RA, Kahvic M (2010) Acute amebic appendicitis: Report of a rare case. Indian Journal of Pathology and Microbiology 53 (4): 767–769.
- Al Omran M, Mandani M, McLeod RS (2003) Epdemiology features of acute appendicitis in Ontario Canada. Canadian Journal of Surgery 46(4): 263-268.
- Mangete ED, Kombo BB (2004) Acute Appendicitis in Port Harcourt, Nigeria Orient Journal of Medicine 16 (1): 1-3.
- Chang AR (1981) An analysis of the pathology of 3003 appendices. Australian and New Zealand Journal of Surgery 51(2): 169-178.
- Freud E, Pilpel D, Mares AJ (1988) Acute appendicitis in childhood in the Negev region: some epidemiological observations over an 11 - year period (1973 - 1983). Journal of Pediatric Gastroenterology and Nutrition 7 (5): 680-684.
- Burkitt DP (1971) The etiology of appendicitis. British Journal of Surgery 58(9): 695-699.
- Walker AR, Segal I (1995) Appendicitis: an African perspective. Journal of The Royal Society of Medicine 88(11): 616-619.
- Oguntola AS, Adeoti MI Oyemolade TA (2010) Appendicitis: Trends in incidence, age, sex, and seasonal variation in South-Western Nigeria. Annals of African Medicine 9 (4): 213-217
- Budd JS Armstrong C (1987) Role of Enterobius vermicularis in the aetiology of appendicitis. British Journal of Surgery 74 (8): 748- 749.
- Yildirm S, Nursa TZ, Tarim A, Kayaselcuk F, Noyan T (2005) A rare cause of acute appendicitis: parasitic infection. Scandinavian Journal of Infection Disease 37(10): 757-759.
- Da silva DF, Da silva RJ, Da silva MG, Sartorelli AC, Rodrigues MA (2007) Parasitic infection of the appendix as a cause of acute appendicitis. Parasitological Research 102(1): 99-102.
- Williams DJ, Dixon MF (1988) Sex, Enterobius vermicularis and the appendix. British Journal of Surgery 75 (12): 1225-1226.
- Villamizar E, Mendez M, Bonill E, Varon H, de Onatra S (1996) Ascaris lumbricoides infection as a cause of intestinal obstruction in children: experience with87 cases. Journal of Pediatric Surgery 31(1): 201-205.
- Cox ND, Yates PJ (2010) Schistosomiasis: a rare cause of acute appendicitis. Journal of Surgical Case Reports 2010(4): 4.
- Akbulut S, Tas M, Sogutcu N, Arikanoglu Z, Basbug M, et al. (2011) Unusual histopathological findings in appendectomy specimens: a retrospective analysis and literature review. The American Journal of Gastroenterology 17(15): 1961-1970.
- Soliman LA (1966) Parasitic lesions of the appendix with reference to their importance in the differential diagnosis of appendicitis. Transactions of The Royal Society of Tropical Medicine and Hygiene 60 (4): 493-496.
- Ossama ZM (2012) The controversy of parasitic infection in pediatric appendicitis: a retrospective analysis. Annals of Pediatric Surgery 8(1): 15-18.
- Doyle PW, Helgason MM, Mathias RG, Proctor EM (1990) Epidemiology and pathogenicity of Blastocystis hominis. Journal of Clinical Microbiology 28(1): 116-121.
- Shilm DR, Hoge CW, Rajah R, Rabold JG, Echeverria P (1995) Is Blastocystis hominisa cause of diarrhea in travelers ? A prospective control study in Nepal. Clinical of Infection Disease Journal 21(1): 97- 101.
- El-Shazly AM, Abdel Magied AA, El Beshbishi SN, El Nahas HA, Fouad MA, et al. (2005) Blastocystis hominis among symptomatic individuals in Talkhacenter, Dakahlin Governorate, Egypt. Journal of Egyptian Society Parasitology 35(2): 653-666.
- Pasupati TM, Yothasamutr K, Wah MJ, Sherif SE, Palayan K (2008) A study of parasitic infection in the luminal contents and tissue sections of appendix specimens. Tropical Biomedicine 25 (2): 166-172.
- Helmy AH, Shousha AT, Magdi M, Sabri T (2000) Appendicitis: appendectomy and the value of endemic parasitic infection. Egyptian Journal of Surgery 19(2): 87- 91.
- Mahdi NH, Mousa AH, Noura AM (2009) Parasitic Appendicitis: A Prospective Clinical and Histopathological Study of 665 Cases of Acute Appendicitis. Journal of Damascus University For Health Sciences 5(1): 87-99.
- Dahlstrom JE, Macarthur EB (1994) Enterobius vermicularis: a possible cause of symptoms resembling appendicitis. Australian and New Zealand Journal of Surgery 64(10): 692-694.
- Aydin O (2007) Incidental parasitic infestations in surgically removed appendices: a retrospective analysis. Diagnostic Pathology 2: 16.
- Efraimidou E, Gatopoulou A, Stamos C, Lirantzopoulos N, Kouklakis G (2008) Enterobius vermicularis infection of the appendix as a cause of acute appendicitis in a Greek adolescent: a case report. Case Journal 1: 376.
- John DT, Petri WA (2006) Markell Voge’s Medical Parasitology. 9th edition. Elsevier Inc. Philadelphia pp: 240-245.
- Salih HA, Sultan BA, Alsai AM (2009) Parasitic cause of acute appendicitis in Najaf. Kufa Medical Journal 12 (2): 62-69.
- Abed Al Rekabi NJ (2010) Parasitic infection accompanying inflammation or bacterial appendicitis in MhavzhzeiQar. Journal De Qar of Science 2(1): 15-21.
