 Research Article
Research ArticleAbstract
Background: Malnutrition is significant factors of deaths of under-five children worldwide, mostly from developing countries. Ethiopia has long history of food insecurity and nutritional problems affecting large proportion of the population caused by successive droughts. Even during the relatively good non-drought seasons, levels of malnutrition in children and women in Ethiopia were extremely high putting the survival of these groups of the population at a greater peril. The most important forms of malnutrition in Ethiopia are macro nutrient deficiency, (vitamin A deficiency, and Iodine deficiency disorders. And the prevalence of wasting, underweight and stunting was very high
Objective: The aim of this study was to evaluate the prevalence, treatment outcomes and determinant factors for of under-five children admitted in Ilu Aba Bor Health facilities therapeutic feeding units with acute Malnutrition.
Methods: Institutional based cross-sectional study was applied. Logistic regression analysis was performed to assess the relation of each determinant of Mal-nutrition treatment outcomes. Statistical significance was defined at a level of 0.05 and data was described with a confidence interval of 95%.
Results and Discussion:361 children were admitted with diagnosis of malnutrition during our study period, within three months. The malnutrition was highly prevalent among 12-36 months age group (44%) and female children; the highly prevalent co morbidities were Pneumonia, anemia and diarrhea with the percentage of 69%, 63% and 58% respectively. Majorities of the under-five children improved during our study period; about 99% of the children admitted with diagnosis of malnutrition improved and discharged. The death rate was 1%. IV fluid administration significantly affects the treatment outcome, in contrast Oral Rehydration Salt (ORS), Rehydration Solution for Malnutrition (ReSoMal), folic acid supplementation and deforming had positive outcome on malnutrition treatment outcomes.
Background
Severe acute malnutrition affects nearly 20 million preschoolage children. Malnutrition is a significant factor in approximately one third of the nearly 8 million deaths in children who are under 5 years of age worldwide [1]. Over 17 million children are affected by severe acute malnutrition (SAM) worldwide. Despite significant progress in recent years, approximately 2.9 million children accessed treatment in 65 countries in 2013 -only about 17 percent of the children needing treatment. Children with SAM are more likely to die than well-nourished children. The management of severe acute malnutrition (SAM) is critical for child survival and is a key cost-effective component of the scaling up nutrition framework for addressing under nutrition [2]. Malnutrition in all its forms is closely linked, either directly or indirectly, to major causes of death and disability worldwide. Understanding the underlying causes of malnutrition should also be factored during the assessment of the situation particularly in geographic areas where SAM burden is particularly high. This information is useful for advocating with relevant actors to address the concerns identified in the assessment or in planning for integration of services with SAM treatment [3]. Every year some 9 million children across the world die before they reach their fifth birthday, and about one-third of these untimely deaths are attributed to under-nutrition. For every child who dies as a result of under-nutrition, there are many millions more who suffer permanent damage to their health; this impairs the rest of their lives.
It appears from the current evidence that malnutrition has a four more powerful impact on children mortality than generally appreciated and strategies combining prevention and treatment a mild to moderate, and severe acute malnutrition will be more effective to address this challenge and reduce its negative impacts [4]. There is high death rates reported from in Ethiopian among children admitted in south Ethiopian Zonal Hospital, the places where severely complicated malnourished were admitted. The death rate is higher in infants under six months of age because of depressed immunity, increased risk of infection and insufficient feeding practices [5]. Evidences of faulty case management practices viz. overuse of intravenous fluids and blood transfusion, inappropriate diets, less use of micronutrients, incorrect antibiotics were observed occasionally in all the three Ethiopian hospitals [6,7]. Maternal under nutrition also contributes to 800 000 neonatal deaths annually; stunting, wasting, and micronutrient deficiencies are estimated to underlie nearly 3.1 million child deaths annually [8,9]. Severe acute malnutrition contributes disproportionately to child mortality rates despite availability of the WHO protocol, “Ten Steps”, to guide hospital management [10,11]. Outpatient Therapeutic feeding Program (OTP) brings the services for management of Severe Acute Malnutrition (SAM) closer to the community by making services available at decentralized treatment points within the primary health care settings [12,13]. Little is known about the program outcomes in south west Ethiopia in general and it is unknown in the study area in particular. This study revealed the levels of program outcome indictors and determinant factors to recovery rate.
Research Questions
1) Whit is the magnitude of Malnutrition of under five children in Ilu Aba Bor Zone areas.
2) What is the fate of under five children affected by Malnutrition and seek treatment in Ilu Aba Bor Zone health facilities.
3) What are the main contributing factors for Malnutrition treatment out comes under-five children in the study areas.
Objective
General Objective
To evaluate treatment practices, treatment outcomes and determinant factors for survival of under five children admitted in Ilu Aba Bor Health facilities therapeutic feeding units with Malnutrition
Specific Objective
To determine Malnutrition treatment practices in Ilu Aba Bor Under five Children To assess treatment outcomes of under- five children affected by Malnutrition in Ilu Aba Bor Zone health facilities To identify determinant factors of treatment outcomes in Ilu Aba Bor Zone Under five children treated children
Method and Material
Study Area and Period
The study was conducted in Ilu Aba Bor Zone Public health facilities. Ilu Aba Bor Zone cover the western part of the region and lies between 34o52’30” E- to36o5’30” E longitudes and 7o27’30” N- 8o49’30” N latitude. The zone characterized by highlands, lowlands, rugged areas, river valley and top flatted plateaus the present land [14].
Study Design
Institutional based cross-sectional study was applied among all patients admitted in pediatrics wards for Mal nutrition in each selected health facility and one patient was followed starting from initiation of therapy until treatment completion In each health facilities appropriate application of all WHO and National guide-line was assessed, the availabilities and types of supplies and practices of Mal-nutrition treatment was evaluated. Three available Hospitals in Ilu Aba Bor Zone was selected purposively(, namely Mettu karl Referral hospital Bedele Zonal Hospital and Darimu District Hospital).For each health facilities two data collector and one supervisor was assign and follow the treatment outcomes at least for two months of working days(60days). Trained data collectors visit the health facility daily and invited patients to participate in the study upon diagnosis of malnutrition. Upon enrollment, data collectors interview each patient care givers to collect demographic, social, and medical information with a structured questionnaire. We used a locally developed and validated scale to determine socioeconomic status. Treatment outcome was obtained from patients’ charts, clinical physical observation. The patient was followed until the completion of sample size.
Sampling Techniques and Sampling Size
All patients diagnosed for Sever acute Malnutrition during the study period and under five age was included in to the study. Then there is no sampling technique was used.
Inclusion and Exclusion Criteria
Inclusion Criteria
Pediatric patients admitted with diagnosis of Sever Acute Malnutrition and age between six months up to five year was included.
Exclusion Criteria
Children with age less than six months and greater than five year was not include to the study. All age children diagnosed other than malnutrition and unwilling parent was also not be included.
Data Quality Control
To evaluate the data collection instrument for its validity of reliabilities and consistency a pilot study was done in Mettu Health center. Training was given for data collectors, the data collected was checked for the completeness, accuracy, by the principal investigator every day and correction was made soon if any fault done.
Data Analysis and Interpretation
All the data was entered, compiled and analyzed by using SPSS current version of statistical software package. A frequency of descriptive statists was presented by using percentages and table. Logistic regression analysis was performed to assess the relation of each determinant of SAM treatment outcomes. The explanatory factors were calculated using multiple logistic regressions. Statistical significance was defined at a level of 0.05 and data was described with a confidence interval of 95%.
Ethical Consideration
Ethical clearance letter was written by University research review board to Zonal health department and to each health institutions and patient care giver willingness also asked.
Results
Totally 361 under five children patients were admitted with malnutrition in selected Ilu Aba Bor health facilities during the study period (January 1 -March 30, 2017). Most of the under five children age 44 %( 160) admitted during the study period were 12-36months and female children in sex 57.89% (160). Regarding the socio economic characterizes of mothers of the under five children admitted with malnutrition during the study period, most of the mothers or care givers 47 %( 171), 63 %( 228), 84 %( 247), 63 %( 228), were illiterate, housewife, married and live in rural resident respectively. 42 %( 251) of the mothers have 3-5 children and 62 %( 227) of them get only <1000 Ethiopian Birr per months (Table 1). Characteristic parameters of children admitted in Ilu Aba Bor health facilities during study period indicated that, most of the children 69.54 %( 159) feed breast milk only for the duration of six months up to twelve months. About 77 %( 260) of the children were fully vaccinated and 18% (57) the children were not totally vaccinated during the study period. Most the children (63%) 228 were admitted with weight for height with >60% and 58 %( 200) were diagnosed with kwashiorkor and new admission (Table 2).
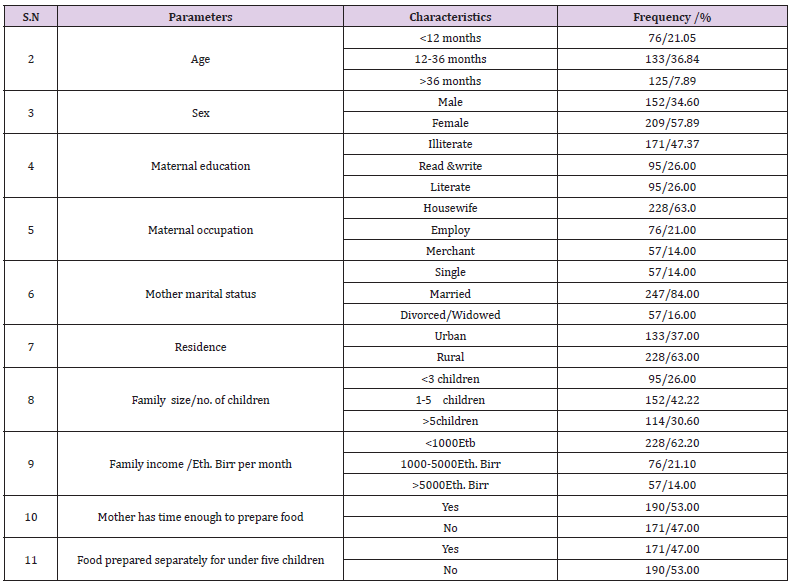
Table 1: Socio -demography characteristics of children’s family or care- givers, during study period in Ilu Aba Bor health facilities.
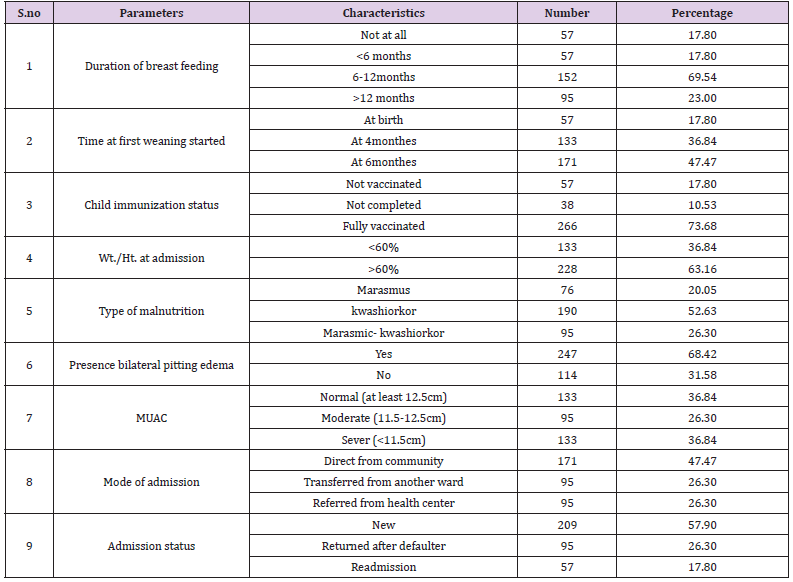
Table 2: Characteristic parameters of children admitted in Ilu Aba Bor health facilities during study period.
More than half of the under-five children admitted in Ilu Aba Bor health facilities were, with diagnosis of malnutrition represented with additional diseases (co-morbidity). Fever, ARTI, Diarrhea, were among the most co-morbidity seen on under-five children admitted in Ilu Aba Bor health facilities with the magnitude of 69%(249), 63%(228) and 58%(209) respectively (Table 3). The major treatment outcomes identified during the study period on under-five children admitted with diagnosis of malnutrition in Ilu Aba Bor health facilities were analyzed as follow : most of the children 68%(246) pass appetite test during the discharge from the feeding units. For most of the admitted children 37 %(132) the first improvement was identified after31 days of admission or above. From the total children admitted with diagnosis of malnutrition in health facility, 1 %( 5) of them were died. Then the death rate was recorded as 1% and cure rate were 99 % (Table 4). IV fluid administration, supplementation of ORS and Rehydration Salt for Malnutrition (ReSoMal) and treatment with routine medications; like folic acid, vitamin ‘A’ supplementation and deforming, were the significant associated factors that determined the treatment outcomes of under-five children admitted with diagnosis of malnutrition in Ilu Aba Bor health facilities during the study period.
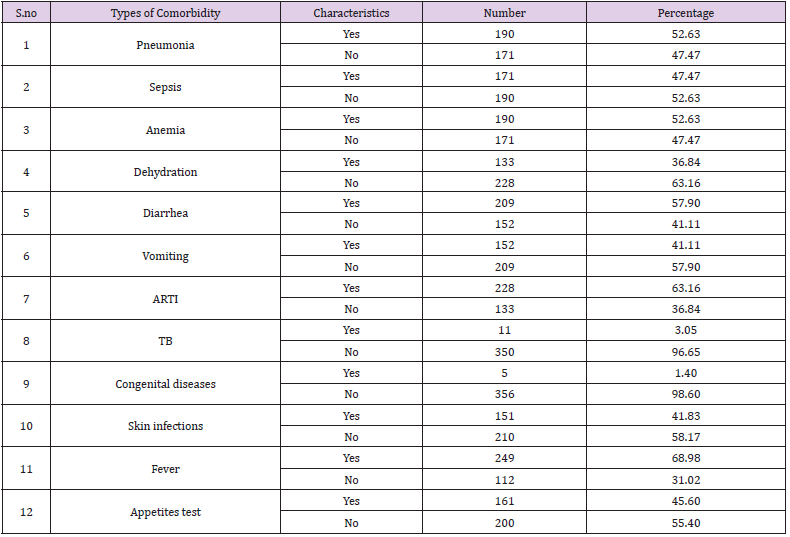
Table 3: Co-morbidity diagnosed with malnutrition on fewer than five children admitted during study period in Ilu Aba Bor health facilities.
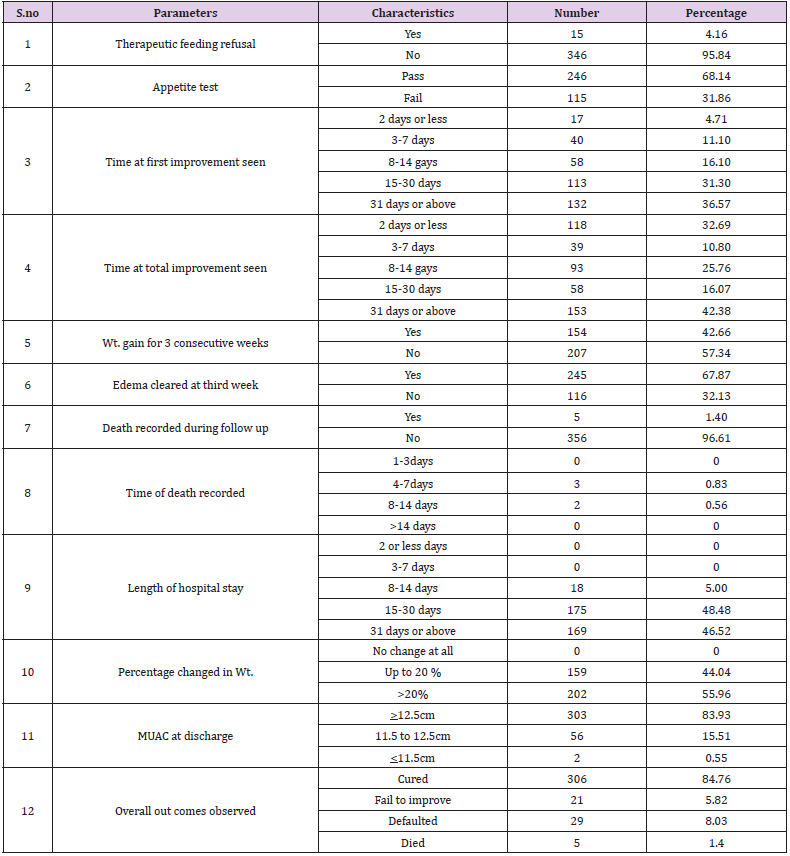
Table 4: Treatment outcomes identified during study period on fewer than five children admitted for malnutrition.
The Odds of IV fluid administration significantly affect the outcome of the treatment 5(95% CI 1.78-12.05) times among patients did not receive it with P-0.034. The Odds of ORS and ReSoMal supplements have good outcomes 6.74(95%CI 2.3-13.20) with P-value0.049 and 5(95%CI 2.31-11.21) with P- value 0.001 times none supplementing of these two solutions respectively. Regarding the routine medication, administration of Amoxicillin antibiotic and supplementation of Vitamin A were not significant in our study with p-value of 0.89 and 0.97 respectively. But the odds of folic acid supplements improve the treatment out comes of malnourished under-five children admitted in Ilu Aba Bor health facilities 5.67(95%CI 2.31-8.93) p-value 0.03 times none supplementing of folic acid. Finally deworming has significant contribution for god outcomes 10.5(95%CI 3.46-15.43) p-value times none supplementing of it (Table 5).
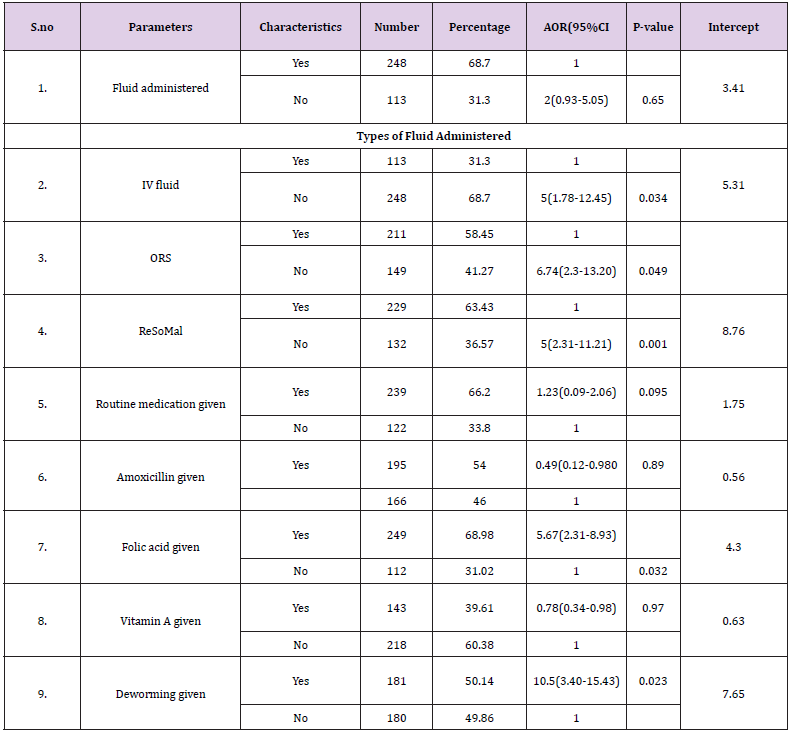
Table 5: Health service practice, base line drugs and supportive treatment related identified factor s during study period in Ilu Aba Bor health facilities
Discussion
Three hundred sixty-one children were admitted in Ilu Aba Bora health facilities with diagnosis of malnutrition during our study period, within three months. The malnutrition was highly prevalent among 12-36 months age group (44%) and female children; this is in line with the study conducted in Bangladeshi during the 2015 [5]. Regarding the characteristic back grounds of under five children, most of the mother, feed their children only breast milk for six months and at least for the duration of one year. This is almost in line with WHO breast feeding guideline [3]. Seventy-seven present of the children were fully vaccinated in Ilu Aba Bor health facilities during our study period and this is much greater than Bangladesh study, Mahamed [5]. This difference may be due to sample size and study period. Almost all under five children admitted with diagnosis of malnutrition during our study period, co morbid with multiple diseases. But the highly prevalent co morbidities were Pneumonia, anemia and diarrhea with the percentage of 69%, 63% and 58% respectively. Majorities of the under-five children improved during our study period; about 99% of the children admitted with diagnosis of malnutrition improved and discharged. The death rate was 1%, this is much less than Bangladesh study, Tabile study (Mohamed sheka et al.) , South region of Ethiopia study (Efirame et al.) and Kamba district study (Negash et al.) [5,13,15].
The determinant factors that affecting the under-five children admitted with diagnosis of was analyzed mainly against health facility related practices like supplementary fluid admiration, routine medication given. Back ward adjusted odd ratio was conducted and identified only the significant factors that affect treatment out comes of under-five malnourished children in our study. Intravenous fluid administration significantly affects the treatment outcome of under-five malnourished children admitted in Ilu Aba Bor health facilities during our study period. In contrast Oral Rehydration Salt (ORS), Rehydration Solution for Malnutrition(ReSoMal), folic acid supplementation and deworming had positive outcome on malnutrition treatment outcomes. The administration of antibiotic (amoxicillin) had no significant effect in our study. This is quaintly different from Yebyo the difference may be due to different in the study site study time and sample size difference and it is in line with Yabeyo et al. regarding deforming effect on under five malnourished treatment outcome [13]. The death rate of our study was 1% this is much less than from Mohamed Saak et al, ashratuddin et al. and Effrem Teferi et al. [5,7,15-18].
Conclusion
This study indicated the basic information of the practices, types of malnutrition family backgrounds, co morbidities, determinant factors and over all treatment outcomes of the under five children admitted with diagnosis of malnutrition in Ilu Aba Bor health facilities. Duration of exclusive breast feeding, immunization coverage, and weight for height personage during admission was in good status in Ilu Aba Bor health facilities. Pneumonia, anemia, diarrhea, Acute Respiratory Tract Infections (ARTI) are among the most prevalent co morbidities seen in study with under five children malnutrition. Kwashiorkor and marasmic kwashiorkor are the most diagnosed in study area during our data collection. Patients with ORS and ReSoMal supplementation more improved and IV fluid administration negatively affect treatment out comes. Deforming and folic acid supplementation also improve the treatment out coms of under-five children malnutrition.
Recommendation
Federal ministry of health, regional health bureau and zonal health office should focus on training of diagnosis, treatment practice, and facilities by special focusing on one to three-year age group. Health facilities should also pay attention beside treatment of malnutrition on identifying and treating of associated co morbidities. Securing IV fluid should be forbidden for manumitted children in health facility; instead ORS and ReSoMal should be supplemented. If ready-made ReSoMal is not available, it should be prepared in health facilities using table salt and sugar based on standard. Further study should be conducted with larger sample size, with long period of time and based severity of malnutrition.
References
- WHO (2013) Updates on the management of severe acute malnutrition in infants and children. World Health Organization Publication.
- UNICEF (2015) Management of Severe Acute Malnutrition in children: Working towards results at scale. Programme Guidance Document.
- WHO (2013 ) Essential Nutrition Actions: improving maternal, newborn, infant and young child health and nutrition. NLM classification: WD 100.
- Zulfiqar A Bhutta, Rizvi A, Gaffey MF, Walker N, Horton S, et al. (2013) Evidence-based interventions for improvement of maternal and child nutrition: what can be done and at what cost?" The Lancet 382(9890): 452-457.
- Ashraf Uddin Ahmed, Taslim Uddin Ahmed, Sultan Uddin, Haider Ali Chowdhury, Mohamnmed Hamidur Rahman, et al. (2013) Outcome of Standardized Case Management of Under-5 Children with Severe Acute Malnutrition in three Hospitals of Dhaka city in Bangladesh." Bangladesh J Child Health 37(1): 5-13.
- Anthony AC (2013) Assessment of clinical practices inchildren admitted with severe acute malnutrition in three District hospitals, in the Western Cape, South Africa. Public Health, University of the Western Cape. Master’s in public health: 115.
- Mahamad Saaka, Shaibu Mohammed Osman, Anthony Amponsem, Juventus B Ziem, Alhassan Abdul Mumin, et al. (2015) Treatment Outcome of Severe Acute Malnutrition Cases at the Tamale Teaching Hospital. Journal of Nutrition and Metabolism 2015: 1-8.
- Desalegn Massa, Kifle Woldemichael, Birtukan Tsehayneh, Amanuel Tesfay (2016) Treatment outcome of severe acute malnutrition and determinants of survival in Northern Ethiopia: A prospective cohort study." International Journal of Nutrition and Metabolism 8(3): 12-23.
- E Teferi, M Lera, S Sita, Z Bogale, DG Datiko, et al. (2010) Treatment outcome of children with severe acute malnutrition admitted to therapeutic feeding centers in Southern Region of Ethiopia. Ethiop J Health Dev 24(3).
- Ahmed DM (2014) Managment Outcome of Severe Acute Malnutrition From 6 Months - 5 Years of age Children admitted to Yekatit 12 Hospital. Medical Faculity Pediatrics and child health addis ababa university P. 1-28.
- Amsalu Bokore Ayana, Tsedeke Wolde Hailemariam, Alemu Sufa Melke (2015) Determinants of acute malnutrition among children aged 6-59 months in Public Hospitals, Oromia region, West Ethiopia: a case-control study. BMC Nutrition 1(34).
- Negash Alemu Shanka, Sebelewengel Lemma, Direslgne Misker Abyu (2015) Recovery Rate and Determinants in Treatment of Children with Severe Acute Malnutrition using Outpatient Therapeutic Feeding Program inKamba District, South West Ethiopia. J Nutr Disorders Ther 5(2).
- Henock Gebremedhin Yebyo, C Kendall, Daniel Nigusse, Wuleta Lemma (2013) Outpatient Therapeutic Feeding Program Outcomes and Determinants in Treatment of Severe Acute Malnutrition in Tigray, Northern Ethiopia: A Retrospective Cohort Study. PLoS ONE 8(6): e65840.
- Delelegn Yilma Gebremichael (2015) Predictors of nutritional recovery time and survival status among children with severe acute malnutrition who have been managed in therapeutic feeding centers, Southern Ethiopia: retrospective cohort study. BMC Public Health 15(1267).
- E Teferi, M Lera, S Sita, Z Bogale, DG Datiko, MA Yassin (2010) Treatment outcome of children with severe acute malnutrition admitted to therapeutic feeding centers in Southern Region of Ethiopia. Ethiop J Health Dev 24(3).
- Lenters LM, Wazny K, Webb P, Ahmed T, Bhutta ZA (2013) Treatment of severe and moderate acute malnutrition in low- and middle-income settings: a systematic review, meta-analysis and Delphiprocess. BMC Public Health 13(S3): 23.
- Ashagrie Terefe Abeje, Temesgen Worku Gudayu, Yewunetu Dessalegn Malefia, Birhanu Boru Befftu (2016) Analysis of Hospital Records on Treatment Outcome of Severe Acute Malnutrition: The Case of Gondar University Tertiary Hospital. Pediatric Therapeut 6: 2.
- (2017) Ilu Ababor Zone Finance and Economic Development office. Physical and socio-economic profile of Ilu Ababor. (Data and Information and physical study of the zone).
