 Case Report
Case ReportAbstract
Rationale: There are several non-cardiac conditions have been reported to mimic these clinical and electrocardiographic changes.
Patient concerns: A 28-year-old Egyptian female patient presented to the emergency room with severe epigastric pain with acute calculous cholecystitis and electrocardiographic ST-segment elevation like-myocardial infarction and bradycardia.
Diagnosis: Acute calculous cholecystitis-induced non-specific ST-segment elevation like-myocardial infarction and bradycardia.
Interventions: Electrocardiography, troponin test, and abdominal ultrasound.
Outcome: Good response after cholecystectomy.
Lessons: Transient spontaneously reversed non-specific electrocardiographic STsegment elevations like-myocardial infarction may happen with calculous cholecystitis. The physician should not hurry to give thrombolytic therapy based on only ST-segment elevations like-myocardial infarction without an accurate decision.
Keywords: Cholecystitis; Induced; Non-Specific ST-Segment Elevation; Like-Myocardial Infarction; Bradycardia
Abbreviations: AMI: Acute Myocardial Infarction; CAD: Coronary Artery Disease; ECG: Electrocardiogram; ICU: Intensive Care Unit
Introduction
Historically, the diseased gallbladder has been accompanied to ECG changes like those of coronary artery disease (CAD) since1878 [1-3]. Chest pain with electrocardiographic changes is usually a fatal presentation of CAD [4]. Numerous non-cardiac conditions that have been reported to mimic the relevant electrocardiographic changes [4]. Many conditions can transiently alter an electrocardiogram. Inflammation of the hepato-biliary system has been noted to produce changes in electrocardiograms [5]. The differential diagnosis of ST-segment elevation is including; ST-elevation of normal variant, early repolarization, left ventricular hypertrophy, left bundle branch block, acute pericarditis, hyperkalemia, Brugada syndrome, pulmonary embolism, cardioversion, Prinzmetal’s angina, and acute myocardial infarction (AMI) [6]. It is possible that acute upper abdominal disease can prematurely reveal sub-clinical changes in the coronary circulation [7]. The changes in the ECG could have been caused by transient CAD since the changes disappeared. However, the exact relevant pathophysiological ECG changes are still unknown mechanism [7]. Acute inflammatory for the gallbladder cause irritation and spasticity of encirclement structures.
This can create reflex stimuli through autonomic pathways to restrict or alter the coronary blood supply may be such that existing minor deficiencies in the coronary circulation become manifest [8]. The reflexive coronary vasoconstriction was unaffected by atropine [9] indicating the reflex has an alpha-adrenergic sympathetic arc [7]. When the initial diagnostic measures for chest pain with STsegment elevation do not results the expected results (with normal cardiac enzyme and an atypical clinical picture), an alternative diagnosis such as cholecystitis should be considered7. These studies examining the ECG effects of biliary abnormality. The ECG changes are usually diffuse, non-specific, T-wave inversions or STsegment depressions [7]. ST-segment elevations are an unusual sign in acute cholecystitis [10]. These electrocardiographic changes are usually reversible with appropriate hepato-biliary management [10]. Despite the ECG changes due to cholecystitis have been shown to be correctable, the relevant pathophysiological changes are still unknown mechanism [4]. The early diagnosis of cholecystitis can establish suitable management and may prevent the achievement of superfluous diagnostic and therapeutic measures [4].
Case Presentation
A 28-year-old married Egyptian female officer patient presented to the emergency room with severe epigastric pain. The epigastric pain referred to both chest and back. The patient was obese. There was associated vomiting. The patient had a history of calculous cholecystitis. Upon examination BP of 130/70mmHg, the pulse of 52bpm, RR of 12bpm, the temperature of 37.7°C, and O2 saturation with pulse oxymetry 99%. There was positive Murphy’s sign. No more relevant clinical data were noted during the clinical examination. The patient was admitted to ICU as chest pain for further assessment. The ECG recordings were showing ST-segment elevation in leads aVL, aVF with reciprocal ST-segment elevation in leads aVR and T-wave inversion in lead II, III, and aVF with VR;52bpm (Figure 1A). ECG recording was taken 33 seconds later showing spontaneous disappearance of above ST-segment elevations with reciprocal ST-segment elevations. This had happened without any medications There was still the presence of T-wave inversions in II, III, and aVF leads (Figure 1B). No electrolytes profile and thyroid function tests abnormalities were detected. The abdominal US showed calculous cholecystitis. The troponin test was below the normal level. Echocardiography was normal. No recurrence for above ECG abnormalities on later serial ECG tracings follows up. Abdominal ultrasound showed multiple variable-sized gallbladder stones with inflammation in the bladder wall. The patient was referred to the surgeon for acalculous cholecystitis management.
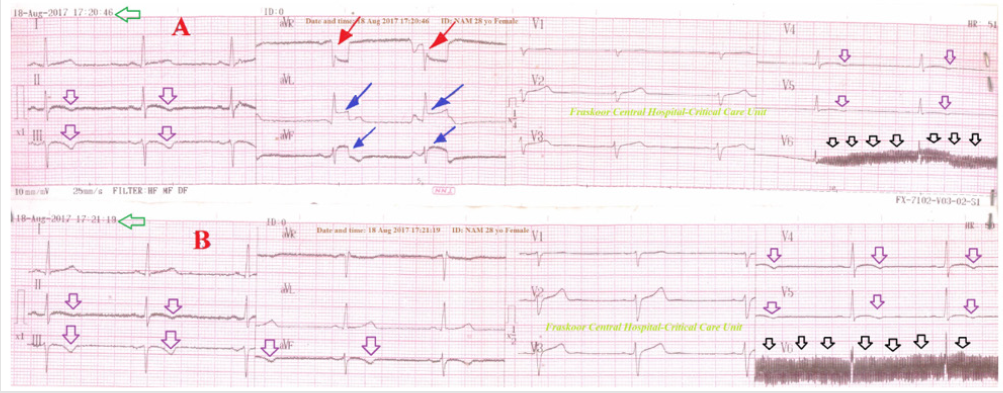
Figure 1: Serial ECG tracings
A. Tracing showing ST-segment elevations in aVL, aVF leads (blue arrows) with reciprocal ST-segment depressions in aVR
lead (red arrows), T-wave inversion in II, III, and aVF leads (purple arrows) with sinus bradycardia (VR;52 bpm), and AC
artifacts in V6 lead (black arrows),
B. Tracing was taken with 33 second of A. tracing showing spontaneous disappearance of above ST-segment elevations
with reciprocal ST-segment elevations. There was still the presence of T-wave inversion in II, III, and aVF leads (purple arrows)
with sinus bradycardia (VR;52 bpm), and AC artifacts in V6 lead (black arrows).
Discussion
Overview
The young patient presented with epigastric pain with electrocardiographic
ST-segment elevations like-AMI in aVL and aVF leads,
reciprocal ST-segment depressions in aVR lead, T-wave inversions
in II, III, and aVF leads, and sinus bradycardia. The ST-segment elevations
like-AMI and reciprocal ST-segment depressions were transient
(disappear within 33 seconds) and non-specific (not coincide
the characteristics of AMI in affected related ECG leads). The patient
was diagnosed as acalculous cholecystitis. Sinus bradycardia
and T-wave inversions reversed after cholecystectomy. I can’t compare
the current case with similar conditions. There are no similar
or known cases with the same management for near comparison.
a. Study Question Here: what are the non-cardiac conditions
that have been reported to mimic these electrocardiographic
changes?
b. The primary objective for my case study was the presence
of transient non-specific ST-segment elevations like-AMI in aVL
and aVF leads with reciprocal ST-segment depressions in aVR
lead.
c. The secondary objective for my case study was the reevaluation
for the actual presence of myocardial infarction
and its subsequent management for immediate reperfusion
therapy.
d. Limitations of the Study: There are no known limitations
in the study.
e. Recommendations: It is recommended to widening the
research in clearing the effect of cholecystitis in inducing mimic
myocardial infarction.
Conclusion
Transient spontaneously reversed non-specific electrocardiographic ST-segment elevations like-myocardial infarction may happen with calculous cholecystitis. The physician should not hurry to give thrombolytic therapy based on only ST-segment elevations like-myocardial infarction without an accurate decision.
Acknowledgment
I wish to thank the critical care unit nurses who make extra ECG copy for helping me.
References
- Breyfogle HS (1940) The frequency of coexisting gallbladder and coronary artery disease. JAMA 114(15): 1434-1437.
- Walsh BJ, Bland EF, Taquini AC, White PD (1941) The association of gall bladder disease and of peptic ulcer with coronary disease: a post-mortem study. Am Heart J 21: 689-697.
- Babcock RH (1909) Chronic cholecystitis as a cause of myocardial incompetence. JAMA 52: 1904 -1911.
- Durning SJ, Nasir JM, Sweet JM, Cation LJ (2006) Chest pain and ST segment elevation attributable to cholecystitis: a case report and review of the literature. Mil Med 171(12): 1255-1258.
- Dickerman JL (1986) Electrocardiographic changes in cardiac patients with acute gallbladder disease. Am Surg 52: 541-543.
- Wang K, Asinger RW, Marriott HJL (2003) ST-Segment Elevation in Conditions Other Than Acute Myocardial Infarction. N Engl J Med 349(22): 2128-2135.
- Patel N, Arun Ariyarathenam, Will Davies, Adrian Harris (2011) Acute Cholecystits Leading to Ischemic ECG Changes in a Patient with No Underlying Cardiac Disease. JSLS 15(1): 105-108.
- Clarice NE (1945) Electrocardiograph changes in active duodenal and gall bladder disease. Am Heart J 29(5): 628-632.
- Vacca G, Battaglia A, Grossini E, Papillo B (1994) Tachycardia and presser responses to dlstention of the gallbladder in the anesthetized pig. Med Sci Res 22: 697-699.
- Peter AD (2017) What is the role of electrocardiography in the diagnosis of cholecystitis?
