 Research Article
Research ArticleAbstract
Introduction: Post-Traumatic Stress Disorder (PTSD) is a common, disabling disorder that appears after the exposure to a traumatic experience. Post-traumatic stress leads to a pattern of symptoms that include a delayed response to an acute stressful and a life-threatening event or situation, such as combat exposure during war time. Individuals exposed to combat exposure in a war zone are not only at risk to experience trauma but typically they may experience multiple traumatic experiences. Gaza Strip was a target for several Israeli aggressions in the last decade. The last and the worst was the offensive of the summer of 2014. People who live in the war zone and were forced to leave their homes have encountered several stressors during the war time that included personal threats to their lives, their families and partial or complete destruction of their homes. Purpose: This study aimed to assess the level of PSTD and to examine the relationship between exposure to war stress and posttraumatic symptoms among people who were forced to leave their homes during/following Israeli offensives against Gaza Strip in 2014.
Methodology: A cross-sectional design was used for this study. The target population of this study was people who were forced to leave their homes during the war. A convenience sample of 190 adults who were forced to leave their homes during the war completed a demographic sheet and Impact Event Scale-Revised (IES-R). IES-R was translated to Arabic in previous studies and proved to be valid and reliable. It has three sub-scales: intrusion, avoidance, and hyper-arousal.Results: The sample consisted of 190 participants, 51.5% (96) of them were males, 13.7% (26) were injured, 18.9% (36) had lost a family member, and 28.9% (55) of them had received psychological support after the event. The results showed that 176 (92.6%) of the participants had scores more than the threshold cut-off point of 35 which means that they have severe posttraumatic symptoms. Total scores of IES-R ranged from 25.03 to 78.0 with a mean of 53.16. The most frequent symptoms of trauma subscales were “Intrusion” (mean=20.94), followed by “Avoidance” (mean=17.66), and then “Hyperarousal” (mean=14.54). Level of trauma symptoms was not affected by sex, place of living, marital status, whether they had experienced an injury, a disability, and home destruction or not. They only factor that had an impact on level of stress was receiving psychological support or not.
Interpretation of Results and Implication for Practice: Despite the long period of the event, the findings of our study showed that participants suffered from severe posttraumatic symptoms four years after the war of 2014 against Gaza Strip. Such high prevalence rates of PSTD will have negative consequences on this group of people including negative health outcomes, social and family relationship, and adverse psychological disorders such as acute depression, anxiety, and psychosocial disorders. This level of trauma warrants intervention programs, including counselling, to reduce stress and trauma among this vulnerable group.
Purpose: This study aimed to assess the level of PSTD and to examine the relationship between exposure to war stress and posttraumatic symptoms among people who were forced to leave their homes during/following Israeli offensives against Gaza Strip in 2014.
Abbreviations: PTSD: Post-Traumatic Stress Disorder; IES-R: Impact Event Scale-Revised; IES: Impact Event Scale; SPSS: Statistical Package for Social Science
Introduction
In the last decade, Israel waged three wars against Gaza Strip. The last war of August 2014 was the worst and the most devastating. It continued for 51 days during July and August 2014. According to a report issued by OCHA (United Nations Office for Coordination of Humanitarian Affairs) which was issued about one week after ceasefire, the war left 2131 deaths (1,473 have been identified as civilians, including 501 children, according to preliminary assessments). About 18,000 housing units were either destroyed or severely damaged, leaving approximately 108,000 people homeless. Moreover, there were approximately 110,000 internally displaced persons who stayed in UNRWA emergency shelters and with host families. Exposure to traumatic events, such as war and displacement from own houses, leads to stress and mental problems [1-3]. According to (Andreasen 2011), such stressors can induce a final common pathway that is expressed by a variety of autonomic/ physiologic, cognitive, and emotional symptoms that occur in response to a severe stressor. Such stressors may lead to a variety of several mental disorders such as depression, anxiety, somatoform disorders, psychosis, substance use disorders, impairment in social functioning, work impairments, and Post-Traumatic Stress Disorder (PTSD) [4-8].
Post-traumatic stress disorder is a common, disabling disorder that appears after the exposure to a traumatic experience [9]. It was defined by (Andreasen 2011) as “a syndrome, defined by a characteristic set of physiological (autonomic) and cognitive and emotional symptoms, that occurs after exposure to severe physical and emotional stress.” Post-traumatic stress leads to a pattern of symptoms that include a delayed response to an acute stressful and a life-threatening event or situation, such as combat exposure during war time [10,11]. These symptoms may appear either during or immediately after the occurrence of the event, or several days later. The symptoms include initially intense fear, helplessness, or horror. Later, the individual develops a response to the stressful event that is characterized by persistently re-experiencing the event, with resultant symptoms of numbness, avoidance and hyperarousal [12]. After exposure to a stressful or a traumatic event, one usually experiences agitation, anxiety and sleep disturbance [13]. Half of those who experience posttraumatic nightmares may have dreams that exactly replicate the traumatic event [13-16]. Moreover, they may have trouble in concentration, and they try to avoid reminders of the event. In the last two decades, research revealed that traumatic events occur far more often than what it was previously assumed [17,18] and that PTSD is a highly prevalent condition with great impact on human and society well-being and costs [19].
PTSD is characterized by three main clusters of symptoms: Re-experiencing, Avoidance, and Hyperarousal symptoms. Reexperiencing symptoms are characterized by intrusive memories, nightmares, flashbacks, and psychological and physiological reactivity when encountering traumatic events. Avoidance symptoms include avoiding thoughts and activities associated with traumatic experiences, inability to recall aspects of the traumatic event, diminished interest, emotional detachment, restricted affect, and a sense of foreshortened future. Hyperarousal symptoms of PTSD include consist of disturbance, irritability/anger, difficulty concentrating, hypervigilance, and an exaggerated startle response [5]. Individuals exposed to combat exposure in a war zone are not only at risk to experience trauma but typically they may experience multiple traumatic experiences [20,21]. Research conducted after various military conflicts has shown that military personnel were subject to considerable risk for mental health problems, including, major depression, substance abuse, impairment in social functioning, work impairments,
PTSD and increased use of health care services [22]. Studies within the Palestinian context related to trauma are limited. They were limited to studying PTSD among children and adolescents [23-30] health care providers [31-34] and a few numbers of studies about adults [36-40]. Despite the abundant studies about PTSD, only a few numbers of them have systematically examined the effect of health care providers and hospital personnel’s exposure to extreme stress [38,39]. In a previous study, we aimed to assess the level of PTSD and to examine the relationship between exposure to war stress and posttraumatic symptoms among health care providers following Israeli offensives against Gaza Strip in 2014. Data were collected three months after the offensives. Results revealed that 89.8% of participants suffered from PTSD. In this study, we aimed to examine if there were any changes of our previous results after two years of the war. People who live in the war zone and were forced to leave their homes have encountered several stressors during the war time that included personal threats to their lives, their families and partial or complete destruction of their homes.
Materials and Methods
A cross-sectional design was used to conduct this study. The target population for the study was all adult individuals who were forced to leave their homes during/following the war of August 2014 against Gaza Strip. A snow-ball technique was used to recruit participants. Organizations that take care of war victims were contacted to recruit participants. Nursing students, friends, and colleagues were asked to recruit participants. The result was a convenience sample of 190 participants. Data were collected in the period between August and December 2018.
Instrument
The Impact Event Scale-Revised (IES-R) [41] was used in this study. The original Impact Event Scale (IES) predated the introduction of the diagnosis of PTSD. It is comprised of 15 items that measure two symptom clusters of PTSDs; seven items measure intrusions and eight items measure avoidance related to a negative event [42-45]. The revision of the original IES was done by Weiss and Marmar to better match the DSM-IV criteria for PTSD. As a result, a third cluster of symptoms that consists of seven items (hyperarousal subscale) was added to the original IES and its now known as IES-R.The IES-R is a self-report questionnaire that consists of 22 items measuring post-traumatic stress symptoms in three clusters: intrusion (seven items), avoidance (eight items) and hyperarousal (seven items). Participants were asked to rate how frequently each symptom was distressing for each participant during the past seven days with respect to the specified potentially stressful event on a 5-point Likert scale (where 0 - not at all, 1= a little bit, 2 = moderately, 3 = quite a bit, and 4 = extremely).
The IES-R has demonstrated good psychometric properties [46]. Briere reported that the internal consistency of the three subscales were found to be very high, with intrusion Cronbach’s alphas ranging from 0.87 to 0.92, avoidance Cronbach’s alphas ranging from 0.84 to 0.86, and hyperarousal Cronbach’s alphas ranging from 0.79 to 0.90. Currently, IES-R is considered one of the most widely used measures to assess posttraumatic stress symptoms [47]. The cut-off score for IES-R varies between 22 and 44 with a score above the cut-off indicating a person at a high risk for psychological problems [48-50]. Considering the variations of cut-off points used in different studies in different groups of participants and different cultures, the investigators chose a cut-off point of 35 for severe posttraumatic symptoms. Choosing a score of 35 as a cut point was because it relatively falls in the middle of the recommended range between 22 and 44. Moreover; it was used in a similar study by Alhajjar, (2014) and in our previous study [51].
The instrument was translated into the Arabic language by two independent bilingual researchers and was used in two previous studies aimed to measure PTSD among health care providers following the 2014 war [52-57]. Then the two Arabic versions were compared, and double checked for accuracy until common agreement about a final translation was agreed upon. Conceptual rather the literal meaning was the goal of the translation. The final Arabic version was then back translated into the English language by a third bilingual researcher. Back-translation is a standard procedure for translating a research questionnaire from English to other languages [58]. Reliability Coefficients (Cronbach’s Alpha) of the Arabic IES-R subscales were: 0.817, 0.779, 0.713 respectively, and 0.892 for total IES-R [59,60].
Statistical Analysis
The Statistical Package for Social Science (SPSS) version 22 was used to analyze data. Data were cleaned and checked for meeting statistical assumptions for normal distribution and homogeneity. Data analysis procedures included basic descriptive statistics (mean, range, standard deviation, and percentage) and frequency distribution tables. ANOVA and t test were used to compare means. Pearson’s correlation was used to test correlations among study variables.
Ethical Considerations
Prior to conducting this research study, approval of the research committee at the Palestinian Ministry of Health was obtained. After explaining the purpose of the study and reassuring participants about confidentiality of data, each participant was asked to sign a consent paper prior to participation.
Results
Characteristics of Participants
The sample consisted of 190 participants. Age of participants ranged between 18 and 75 years with a mean of 28.75 (±10.55) and 96 (51.5%) of t were males. Only 26 (13.7%) participants reported that they were injured during the war. One participant (3.7%) described his injury as severe while the others described their injuries as moderate (n= 18, 66.7%) or mild (n=8, 29.6%). 36 (18.9%) had lost a family member. Only 29 (15.7&) participants reported that their houses were not destroyed while 109 (58.9%) reported partial destruction of their houses and 46 participants had a complete destruction of their houses. Finally, only 55 (28.9%) of the participants had received psychological support after the event. Table 1 summarizes demographic characteristics of the participants.
Analysis of IES-R Scale
The results of our study revealed that the great majority of the participants (N=174, 91.6%) had scores more than 35 (threshold cut-off) on IES-R scale. The mean for the total score of IES-R scale was 53.12 (±10.92) and values ranged between 25.03 and 78.0. Table 2 summarizes the results of the IES-R scale and its subscales. The highest mean of the subscales belongs to “Intrusion” (mean=20.95) followed by “Avoidance” (mean=17.66) while the least frequently reported symptoms were related to hyper arousal subscale (mean=14.54). Table 3 shows the results for each item of the IES-R scale. The highest scores for the most stressful symptoms of trauma, as ranked by the participants, were “I had waves of strong feelings about it” (mean=3.24), followed by “I felt watchful or on-guard” (mean=3.03), and “Pictures about it popped up into my mind” (mean=3.03). The least frequent symptoms of trauma were “Reminders of it caused me to have physical reactions, such as sweating, trouble breathing, nausea or a pounding heart” (mean=1.70) and “My feelings about it were kind of numb” (mean=1.72).
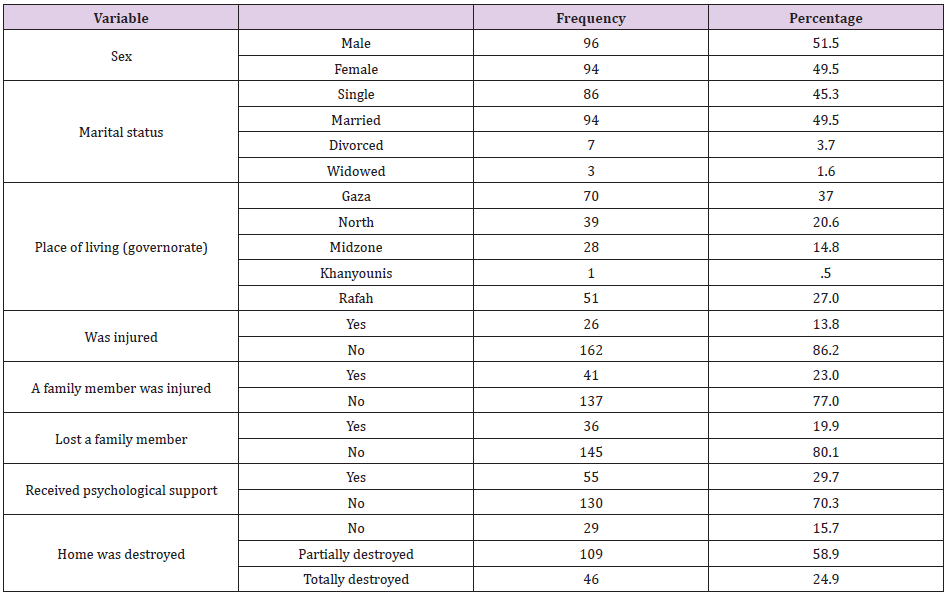
Table 1: Characteristics of participants.

Table 2: Means and standard deviations of trauma symptoms by subscales.
Association Between Study Variables and PTSD
Table 4 depicts the association between study variables and IES-R scores and its sub-domains. Independent t test revealed that there were no statistically significant differences between the means of IES-R score or its subdomains among participants in many variables including sex, marital status, or was injured or not during the war (Table 4). On the other hand, variables such as having a family injured, losing a family member and receiving psychological support were found to have impact on IES-R score and all or some of its domains. Moreover, ANOVA test revealed that place of living and degree or home destruction had no impact on IES-R score and its domains. Correlation results revealed that there was no correlation between age of participants and total IES-R and its three subscales.
Discussion
This study reveals that people who were displaced from their homes during the 2014 war still suffer from PTSD after four years of the war. Our results revealed that 91.6% had a score of more than 35 (the cut-off point) on the IES-R scale. The levels of PTSD reported in this study are amongst the highest levels reported in other parts of the world who were affected by wars and other armed conflicts. For example, rates of PTSD among Guatemalan refugees in Mexico were reported at 11.8% of the participants after 20 years of the war and 4.6% among Karenni refugees living in the Thai-Burma border [61- 63]. Studies about level of PTSD among participants from Bosnian refugees in Croatia varied from 26.3% [64] three years after the war to 5.6% [65] about 20 years after the war. Another study from Bosnia found that 18.6% of individuals in the resident’s sample, 32.7% of those in medical treatment, and 38.6% of those receiving psychological treatment developed PTSD [66,67]. Similarly, rates of PTSD among participants from Afghanistan have varied between 20.4% (Scholte et al. 2004) to 42%.
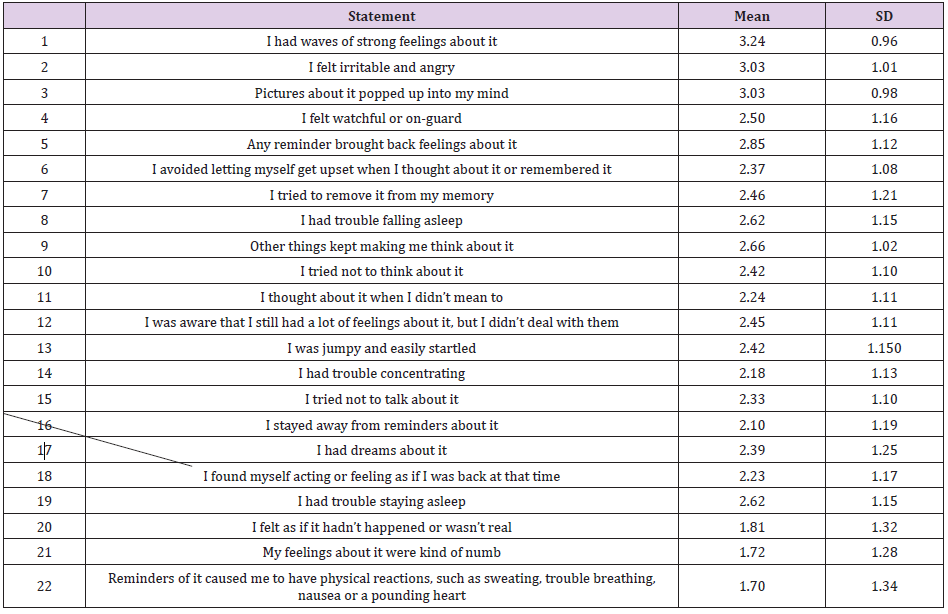
Table 3: Mean values of the concentration in NO2 and PM10 in the Campus.
In a different cross-sectional study that was conduct in the town of Juba, (2 years after the end of the civil conflict in Sudan), results revealed that over one third (36%) of respondents met symptom criteria for PTSD. Another study that assessed level of PTSD of residents from South Sudan revealed 48% of residents in southern Sudan and 46% of refugees from southern Sudan living in Uganda had PTSD. Although that our study reported the highest level of PTSD, other several studies had reported similarly high rates of PTSD among civilians forced to leave their homes and areas of conflict. In their study, Roberts et al. found that more than 54% of participants who were forced to leave their area of living in Uganda during armed conflict met the criteria for PTSD and more than 67% of them met symptom criteria for depression. The results of Vinck et al. showed also that a high percentage of participants (74.3%) met PTSD symptom criteria and 44.5% met depression symptom criteria among Ugandans during armed conflicts. Dahl et al. found that the proportion of PTSD among women who had survived the most severe traumas (concentration camps or other kinds of detention) in Bosnia was as high as 71% of participants.
Factors influenced that the rate of PSTD among these women were high numbers of traumas, having children, being over 25 years of age, and reporting of an absent husband Dahl et al. The reasons for this unusual high level of PTSD among our participants could be due to one or two reasons. Firstly, the participants live on the border side between Gaza Strip and Israel where there are continuous harassments from the Israelis, which put continuous pressure and threats on the people living in this area. Examples of Israeli harassments include shooting at any person who gets close to the borders, limited invasions into the Palestinian side and bombardments of certain targets on the Palestinian side. Such act results occasionally in injuring or killing some of the Palestinians living near the borders. The second reason could be due to the Great Marsh of Return activities which started on March 30, 2018, a few months before starting our data collection. Since that time, Palestinians gathered on a weekly basis (each Friday) at the Palestinian side of the Palestinian-Israeli border line.
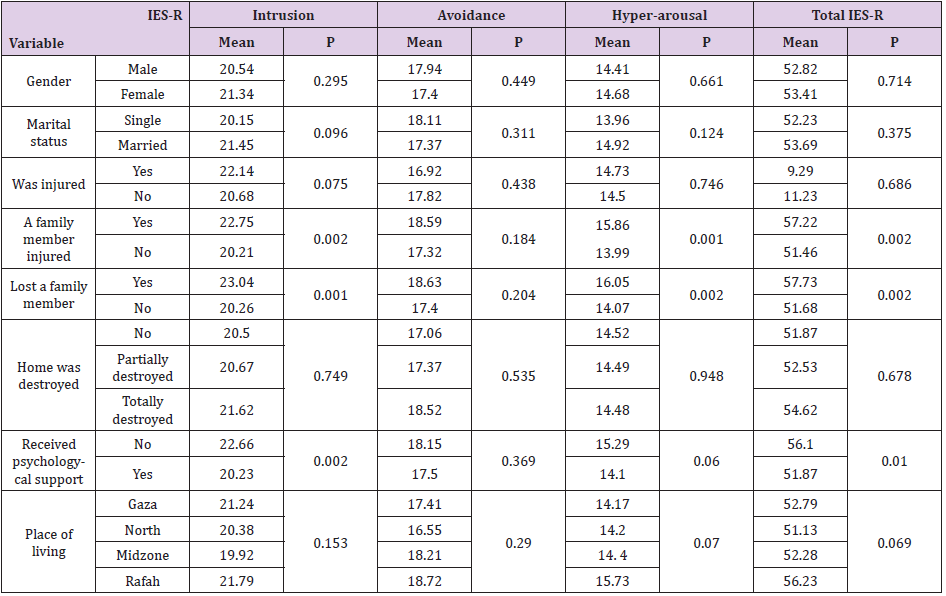
Table 4: Comparison of IES-R and its subscales in relation to different variables.
The Israelis respond to this assembly by shooting at the Palestinians and throwing gas bombs against them. The latest report issued by the ministry of health on March 9th, 2019 revealed that 261 Palestinians were killed and 29,678 were injured). Such a high number of deaths and casualties leave people who are living in the area under constant pressure and constant threat to be killed or injured themselves or a family member which may contribute to the high level of PTSD reported in this study. Moreover, the results of this study showed that the level of PTSD among people from Gaza Strip who were forced to leave their homes were higher than those reported by health care professionals immediately after the same war and two years after the same war. This can be due to the fact that health care professionals (especially doctors) are getting familiar to deal with such stressful situations and dealing with cadavers and other badly injured people which help them to develop coping strategies which resolved in higher resilience during the exposure to victims during war time.
The study did not find significant associations of all independent variables, such as gender, marital status, etc. (Table 4) on the rate of PTSD. One exception was the variable receiving psychological support or not. Participants who received psychological support reported less scores of PTSDs in all the domains of IES-R, but these scores were statistically significant for intrusion domain (p = 0.002) and for the total IES-R score (P = 0.010). This result, along with other findings from other studies, emphasize the importance of providing psychological support for this vulnerable individual who are at consistent and continuous pressure and distress due to the on-going conflict at the Palestinian-Israeli borders. The highest scores of the IES-R went to the intrusion subscale (20.85) followed by avoidance (17.66) and hyper-arousal received the least score (14.54). These findings wear in line with other studies which reported that avoidance was the most prominent symptom followed by avoidance and hyper-arousal among health care providers who witnessed the 2008 and 2014 wars against the Gaza Strip.
Conclusion
Results of this study revealed a very high level of PTSD among Palestinians who were forced to leave their homes four years after the 2014 war. The reported rate of PTSD is one of the highest levels reported in global literature. PTSD has a negative sequel on mental health. For example, it leads to depression and dysphoria, increased anger level, family distress and troubled family relationships and secondary traumatization among family members and social dysfunction. The presence of high numbers of PTSD cases requires the implementation of individual and community-based treatment programs to protect them and promote their mental health. Examples of treatment programs include sessions of supportive counseling and psychoeducation. Many programs that provide psychosocial support, especially those implemented by local personnel, showed promising outcomes and were effective to reduce the impact of PTSD. Moreover Hyman, Gold and Cott added that social support had significantly buffered PTSD development. Based on that, the researchers recommend the implementation of such supportive programs to buffer PTSD and limit its impact on mental health of people living on war zones.
References
- Abdelaziz T, T Abdulla, P Vostanis (2013) Coping strategies of children and adolescents exposed to war conflict.
- Abu El Noor NI, YI Aljeesh, AK S Radwan, MK Abu El Noor, IAI Qddura (2018) Post-traumatic Stress Disorder Among Health Care Providers Two Years Following the Israeli Attacks Against Gaza Strip in August 2014: Another Call for Policy Intervention. Archives of psychiatric nursing 32(2): 188-193.
- Abu El Noor NI, YI Aljeesh, AS Radwan, MK Abu El Noor, IA I Qddura, et al. (2016) Post-traumatic stress disorder among health care providers following the Israeli attacks against Gaza Strip in 2014: a call for immediate policy actions. Archives of psychiatric nursing 30(2): 185-191.
- Al Sheikh NA M, AA M Thabet (2017) Post-Traumatic Stress Disorder due to War Trauma, Social and Family Support among Adolescent in the Gaza Strip. J Nurs Health Sci 3: 10.
- Al Ghalayini H, AM Thabet (2017) The Relationship between War Trauma and Anxiety and Posttraumatic Stress Disorder among Preschool Children in the Gaza strip. Arab Journal of Psychiatry 28.
- Alhajjar B (2014) Gaza nurses after war: Are they traumatized? Procedia-Social and Behavioral Sciences 114: 802-809.
- (2000) American Psychiatric Association. Diagnostic and statistical manual of mental disorders. Washington, DC: American Psychiatric Association.
- Andreasen NC (2011) What is post-traumatic stress disorder? Dialogues in clinical neuroscience 13: 240.
- Ben Ezra M, Y Palgi, N Essar (2007) Impact of war stress on posttraumatic stress symptoms in hospital personnel. Gen Hosp Psychiatry 29(3): 264-266.
- Biehn TL, A Contractor JD Elhai, M Tamburrino, TH Fine, MR Prescott (2013) Relations between the underlying dimensions of PTSD and major depression using an epidemiological survey of deployed Ohio National Guard soldiers. Journal of Affective Disorders 144(1-2): 106-111.
- Blanc J, E Bui, Y Mouchenik, D Derivois, P Birmes (2015) Prevalence of post-traumatic stress disorder and depression in two groups of children one year after the January 2010 earthquake in Haiti. Journal of affective disorders 172: 121-126.
- Briere J (1977) Psychological assessment of adult posttraumatic states. Washington, DC: American Psychological Association.
- Cardozo BL, OO Bilukha, CAG Crawford, I Shaikh, MI Wolfe, et al. (2004a) Mental health, social functioning, and disability in postwar Afghanistan. Jama 292(2): 575-584.
- Cardozo BL, L Talley A Burton, C Crawford (2004b) Karenni refugees living in Thai–Burmese border camps: traumatic experiences, mental health outcomes, and social functioning. Social science & medicine 58(12): 2637-2644.
- Dahl S, A Mutapcic, B Schei (1998) Traumatic events and predictive factors for posttraumatic symptoms in displaced Bosnian women in a war zone. Journal of Traumatic Stress: Official Publication of The International Society for Traumatic Stress Studies 11(1): 137-145.
- Davis J, P Byrd, J Rhudy, D Wright (2007) Characteristics of chronic nightmares in a trauma-exposed treatment-seeking sample. Dreaming 17(4): 187-198.
- Dekel R, CM Monson (2010) Military-related post-traumatic stress disorder and family relations: Current knowledge and future directions. Aggression and Violent Behavior 15(4): 303-309.
- Dyregrov A, R Gjestad (2003) A maritime disaster: reactions and follow-up. Int J Emerg Ment Health 5(1): 3-14.
- Elhai JD, MJ Gray, TB Kashdan, CL Franklin (2005) Which instruments are most commonly used to assess traumatic event exposure and posttraumatic effects? A survey of traumatic stress professionals. J Trauma Stress 18(5): 541-545.
- Galovski T, JA Lyons (2004) Psychological sequelae of combat violence: A review of the impact of PTSD on the veteran's family and possible interventions. Aggression and violent behavior 9(5): 477-501.
- Hall BJ, SM Murray, S Galea, D Canetti, SE Hobfoll (2015) Loss of social resources predicts incident posttraumatic stress disorder during ongoing political violence within the Palestinian Authority. Social psychiatry and psychiatric epidemiology 50(4): 561-568.
- Hodgetts G, T Broers, M Godwin, E Bowering, M Hasanovic (2003) Post-traumatic stress disorder among family physicians in Bosnia and Herzegovina. Fam Pract 20(4): 489-491.
- Hollifield M, TD Warner, N Lian, B Krakow, H Jenkins, et al. (2002) Measuring trauma and health status in refugees: a critical review. Jama 288(5): 611-621.
- Horowitz M, N Wilner, W Alvarez (1979) Impact of Event Scale: a measure of subjective stress. Psychosom Med 41(3): 209-218.
- Hyman SM, SN Gold, MA Cott (2003) Forms of social support that moderate PTSD in childhood sexual abuse survivors. Journal of Family Violence 18: 295-300.
- Karunakara UK, F Neuner, M Schauer, K Singh, K Hill, et al. (2004) Traumatic events and symptoms of post-traumatic stress disorder amongst Sudanese nationals, refugees and Ugandans in the West Nile. African health sciences 4(2): 83-93.
- Kessler RC (2000) Posttraumatic stress disorder: the burden to the individual and to society. J Clin Psychiatry, 61(Suppl 5): 4-12.
- Khamis V (2015) Coping with war trauma and psychological distress among school-age Palestinian children. American journal of orthopsychiatry 85(1): 72.
- Kim HS, D Schwartz Barcott, IM Holter, M Lorensen (1995) Developing a translation of the McGill pain questionnaire for cross-cultural comparison: an example from Norway. J Adv Nurs 21(3): 421-426.
- Lavoie S, LR Talbot, L Mathieu (2011) Post-traumatic stress disorder symptoms among emergency nurses: their perspective and a 'tailor-made' solution. J Adv Nurs 67(7): 1514-1522.
- Luce A, J Firth Cozens, S Midgley, C Burges (2002) After the Omagh bomb: posttraumatic stress disorder in health service staff. J Trauma Stress 15(1): 27-30.
- McCarthy S (2001) Post-traumatic stress disorder in people with learning disabilities. Advances in Psychiatric Treatment 7(3): 163-169.
- McInnes K, N Sarajlić, J Lavelle, I Sarajlić (1999) Disability associated with psychiatric comorbidity and health status in Bosnian refugees living in Croatia. Jama 282(5): 433-439.
- (2019) Ministry of Health. A special report about Israeli agression againist participants of Peaceful Marsh of Return. Gaza.
- Nemeroff CB, JD Bremner, EB Foa, HS Mayberg, CS North (2006) Posttraumatic stress disorder: a state-of-the-science review. J Psychiatr Res 40(1): 1-21.
- Neuner F, M Schauer, C Klaschik, U Karunakara, T Elbert (2004) A comparison of narrative exposure therapy, supportive counseling, and psychoeducation for treating posttraumatic stress disorder in an african refugee settlement. Journal of consulting and clinical psychology 72(4): 579.
- Nosè M, F Ballette, I Bighelli, G Turrini, M Purgato, et al. (2017) Psychosocial interventions for post-traumatic stress disorder in refugees and asylum seekers resettled in high-income countries: Systematic review and meta-analysis. PloS one, 12(2): e0171030.
- (2014) OCHA. Occupied Palestinian Territory: Gaza Emergency Situation Report (as of 4 September 2014, 08:00 hrs). Office for the Coordination of Humanitarian Affairs.
- Onyut LP, F Neuner, E Schauer, V Ertl, M Odenwald (2004) The Nakivale Camp Mental Health Project: Building local competency for psychological assistance to traumatised refugees. Intervention 2: 90-107.
- Powers MB, JM Halpern, MP Ferenschak, SJ Gillihan, EB Foa (2010) A meta-analytic review of prolonged exposure for posttraumatic stress disorder. Clinical psychology review 30(6): 635-641.
- Punamäki RL, E Palosaari, M Diab, K Peltonen, SR Qouta (2015) Trajectories of posttraumatic stress symptoms (PTSS) after major war among Palestinian children: Trauma, family-and child-related predictors. Journal of affective disorders 172: 133-140.
- Risser HJ, MD Hetzel Riggin, CJ Thomsen, TR McCanne (2006) PTSD as a mediator of sexual revictimization: the role of reexperiencing, avoidance, and arousal symptoms. J Trauma Stress 19(5): 687-698.
- Roberts B, EY Damundu, O Lomoro, E. Sondorp (2009) Post-conflict mental health needs: a cross-sectional survey of trauma, depression and associated factors in Juba, Southern Sudan. BMC psychiatry 9: 7.
- Roberts B, KF Ocaka, J Browne, T Oyok, E Sondorp (2008) Factors associated with post-traumatic stress disorder and depression amongst internally displaced persons in northern Uganda. BMC psychiatry 8: 38.
- Rosner R, S Powell, W Butollo (2003) Posttraumatic stress disorder three years after the siege of Sarajevo. Journal of Clinical Psychology 59(1): 41-55.
- Rossignol M, H Chandler (2010) Recognising posttraumatic stress disorder in military veterans. American Nurse Today 5: 2.
- Sabin M, BL Cardozo, L Nackerud, R Kaiser, L Varese (2003) Factors associated with poor mental health among Guatemalan refugees living in Mexico 20 years after civil conflict. Jama 290(5): 635-642.
- Scholte WF, M Olff, P Ventevogel, GJ de Vries, E Jansveld, et al. (2004) Mental health symptoms following war and repression in eastern Afghanistan. Jama 292(5): 585-593.
- Schweitzer R, F Melville, Z Steel, P Lacherez (2006) Trauma, post-migration living difficulties, and social support as predictors of psychological adjustment in resettled Sudanese refugees. Australian & New Zealand Journal of Psychiatry 40(2): 179-187.
- Shamia N, A Thabet, P Vostanis (2015) Exposure to war traumatic experiences, post‐traumatic stress disorder and post‐traumatic growth among nurses in Gaza. Journal of psychiatric and mental health nursing, 22(10): 749-755.
- Thabet A, O El Buhaisi, P Vostanis (2014) Trauma, PTSD, Anxiety, and coping strategies among Palestinians adolescents exposed to War on Gaza. The Arab Journal of Psychiatry 25: 71-82.
- Thabet A, M Elheloub, P Vostanis (2015a) Exposure to war traumatic experiences, post traumatic growth and resilience among university students in Gaza. American Journal of Advanced Medical Sciences (AJAMS) 1: 1-8.
- Thabet A, AA Tawahina, R Punamäki, P Vostanis (2015b) Prevalence and mental health function of resilience in condition of military siege and violence in a palestinian community sample. Journal of Psychiatry 18: 1-9.
- Thabet A, S Thabet (2015) Trauma, PTSD, anxiety, and resilience in Palestinian children in the Gaza strip. British Journal of Education Society & Behavioural Science 11: 1-13.
- Thabet AA, P Vostanis (2000) Post traumatic stress disorder reactions in children of war: a longitudinal study. Child abuse & neglect 24(2): 291-298.
- Thabet AM (2018) The Relationship Between Trauma Due to War, Post Traumatic Stress Disorder and Fears among Palestinian Children. EC Paediatrics 7: 171-178.
- Thabet AM, SS Thabet (2017) Stress, trauma and post-traumatic stress disorder among adolescents in the Gaza strip. Journal of Trauma and Critical Care 1(2): 25-33.
- Thabet AM, SS Thabet, P Vostanis (2016) The relationship between war trauma, PTSD, depression, and anxiety among Palestinian children in the Gaza Strip. Health Science Journal 10: 1.
- Tol WA, C Barbui, A Galappatti, D Silove, TS Betancourt, et al. (2011) Mental health and psychosocial support in humanitarian settings: linking practice and research. The Lancet 378(9802): 1581-1591.
- Tufan, AE, M Alkin, S Bosgelmez (2013) Post-traumatic stress disorder among asylum seekers and refugees in Istanbul may be predicted by torture and loss due to violence. Nordic journal of psychiatry 67(3): 219-224.
- Vinck P, PN Pham, E Stover, HM Weinstein (2007) Exposure to war crimes and implications for peace building in northern Uganda. Jama 298(5): 543-554.
- Vuković IS, N Jovanović, B Kolarić, V Vidović, RF Mollica (2014) Psychological and somatic health problems in Bosnian refugees: A three-year follow-up. Psychiatria Danubina, 26(Suppl 3): 306-444.
- Weathers FW, TM Keane (2007) The Criterion A problem revisited: controversies and challenges in defining and measuring psychological trauma. J Trauma Stress 20(2): 107-121.
- Weiniger CF, AY Shalev, H Ofek, S Freedman, C Weissman (2006) Posttraumatic stress disorder among hospital surgical physicians exposed to victims of terror: a prospective, controlled questionnaire survey. Journal of Clinical Psychiatry 67(6): 890-896.
- Weiss, Daniel S (2004) The Impact of Event Scale-Revised. In Assessing psychological trauma and PTSD: A practitioner’s handbook. In: JP Wilson, TM Keane (Eds.), Guilford press, New York, USA Pp: 168-189.
- Weiss D, C Marmar (1997) The Impact of Event Scale-Revised. In Assessing psychological trauma andPTSD. In J Wilson, T Keane (Eds.), Guilford press, New York, USA, pp: 399-411.
- Wittmann L, M Schredlm, M Kramer (2007) Dreaming in posttraumatic stress disorder: A critical review of phenomenology, psychophysiology and treatment. Psychotherapy and Psychosomatics 76(1): 25-39.
