 Case Report
Case ReportABSTRACT
Necrobacillosis is a life-threatening and not so unusual illness. Also called Lemierre syndrome, septic thrombophlebitis of the internal jugular vein with metastatic infection occur after pharynx and peritonsillar tissue infections. Fusobacterium necrophorum, a strict anaerobic bacteria, is still the main agent of the syndrome. Here we report a healthy 23-year-old woman with signs of sepsis and dyspnea, following 2 weeks of an apparent uncomplicated pharyngitiswich was treated with five days of azithromycin. The diagnosis was suggested by cervical mass and thrombosis of the left jugular internal vein showed by bedside ultrasonography. Outlined by this case report, we highlight the signs, the symptoms and the management of Lemierre syndrome which requires high clinical suspicion and immediate treatment, otherwise it may lead to death.
Keywords: Lemierre Syndrome; Necrobacillosis; Fusobacterium Necrophorum; Sepsis Postanginal
Introduction
The Lemierre syndrome, described in 1936 [1] is characterized by pharyngitis and peritonsilite complicated by septic internal jugular vein thrombosis and metastatic infections. The original description and most cases have been related to hematogenous dissemination of Fusobacterium necrophorum, a strict anaerobic bacteria. Since widespread use of antibiotics, the disease has become extremely rare, even though new reports have been emerged in the last two decades [1,2]. The objective is to present a Lemierre syndrome case treated at University Hospital highlighting for this rare syndrome that should not be overlooked.
Case Report
A 23-year-old white woman has admitted to the hospital with a history of fever and refractory low back pain irradiated to right leg for seven days. She described sore throat treated with five days of azithromycin two weeks before hospital admission. Her medical history was unremarkable, and she denies any illicit drug or smoking. Pharyngitis last for only seven days but highintensity lumbar pain, dyspnea, left neck mass, and fever up to 39 °C coming on. At the time of presentation, the patient was 38.4 °C, hypoxic and dyspneic (respiratory rate of 32 per minute). The heart rate was 112 beats per minute and blood pressure was 112/68 mmHg. She presented severe pain in the hip and lower back radiating to the right leg. On examination, mild erythema in the oropharynx, painful left neck abscess with lymphadenitis around this neck mass were noticed. There are inaudible breath sounds and dullness to percussion on the left hemithorax. Laboratory investigations revealed mild normocytic normochromic anemia, elevated inflammatory markers as C-reactive protein, erythrocyte sedimentation rate and neutrophilic leukocytosis. Serum creatinine and liver function tests were within normal range.
A chest radiograph showed large free left pleural effusion. Blood cultures were collected and Piperacillin-tazobactam was initiated for sepsis. The patient was submitted to computed tomography (CT) image of neck and chest that showed collection on the left side of neck spreading from the parapharyngeal space to the supraclavicular region. The left internal jugular vein could not be visualized because bulky collection was hindering it. Lung CT images showed up large left pleural effusion and multiple bilateral pulmonary nodular opacities, some excavated, with soft tissue density measuring 8 to 13mm, suggesting an embolic origin (Figure 1). Abdomen and pelvis CT demonstrated an unexpected iliopsoas abscesses, mainly on the right side. The patient was promptly submitted to needle aspiration of cervical mass and diagnostic thoracentesis, but later the exudative pleural effusion was drained. Doppler ultrasound of cervical mass and veins revealed thrombosis within left internal jugular vein. The patient proceeded to the operating room for neck and iliopsoas abscesses drainage. Cultures of neck collection, pleural effusion, iliopsoas abscesses and blood were carried out to detect common germs, fungi and mycobacteria. Despite the negative tests, classical clinical picture and the improvement with antibiotic were essential to make the diagnosis. Venous therapy was maintained for two weeks and oral therapy with metronidazole for complete six weeks. The young patient was discharged without residual disability.
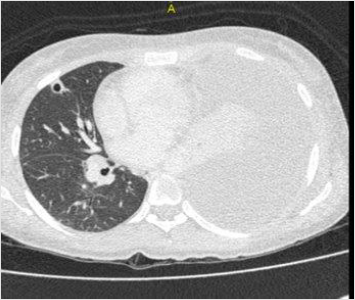
Figure 1: Large left pleural effusion and multiple bilateral pulmonary nodular excavated opacities.
Discussion
Currently, the term Lemierre syndrome is more commonly used as a clinical diagnosis when thrombophlebitis and post-anginal sepsis occur [3]. The estimated incidence is from 1 to 3.6 cases per million affecting mainly young people, between 10 and 35 years [4], without diseases or immunosuppressive conditions [5,6]. The high mortality initially described around 90% [7], significantly declined by the advent of antibiotics [2]. As result, the number of cases has also decreased, underestimating the real incidence of Lemierre syndrome. The Fusobacterium necrophorum remains the primarily responsible in around 80% of cases which has the streptococcus and staphylococcal groups as secondary causes [2,4]. Unfortunately, we may not isolate the pathogen, but it is not strictly necessary to characterize the syndrome. There are difficulties in the cultures techniques and the slow growing of bacteria, allow us prompt treatment. The increase in reported cases seems to result from reluctance to start antibiotics for uncomplicated pharyngitis although being a good practice, and the routine use of macrolides that have no action against Fusobacterium sp. Furthermore, increased clinical awareness, improved blood culture techniques for F. necrophorum detection, added to availability of imaging to detect thrombosis of the internal jugular vein, significantly enhance the reports [1].
The infection come up from the oropharyngeal and tonsils leading to septic thrombophlebitis and abscesses [1]. After the development of thrombophlebitis, haematogenous or lymphatic dissemination from peritonsillar vessels leads to impairment of the lung and pleura in over 90% of cases, followed by joints, skin, soft tissue and liver [4]. The most common symptom is sore throat and the most specific clinical sign of the syndrome is swelling or pain especially in the internal jugular vein territory, present in 52% of patients as occurred (Figure 2) [2]. Proper management of patients with suspected Lemierre syndrome is done by a high grade of suspicion, imaging studies, culture, long-term antibiotic therapy against Fusobacterium and drainage of collections when indicated [8]. As there is no consensus about antibiotic regimens, it is guided by expert’s experience, advising six weeks of therapy [4]. Thus, due to the Fusobacterium resistance to penicillin, commonly used antibiotics are: penicillin and beta-lactamase inhibitor, carbapenem, or in case of penicillin allergy, metronidazole [4,9]. Anticoagulation is controversial because of the lack prospective studies. When there is an neck surgery indication, the thrombosed vein should be removed [8].
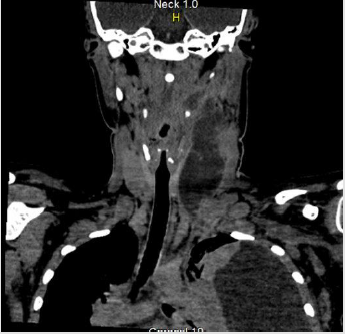
Figure 2: Cervical CT with cervical swelling.
Conclusion
Lemierre syndrome is a potentially fatal disease that should be suspected in young patients with recent pharyngitis history developing persistent fever despite the common antibiotic therapy. The differential diagnosis is broad and may lead to delay in treatment. Therefore, the beginning of antibiotics, especially against anaerobic, should not be postponed otherwise may increase morbidity and mortality.
References
- Gupta T, Parikh K, Puri S, Agrawal S, Agrawal N, et al. (2014) The forgotten disease: Bilateral lemierre’s disease with mycotic aneurysm of the vertebral artery. Am J Case Rep 15: 230-234.
- Karkos PD, Asrani S, Karkos CD, Leong SC, Theochari EG, et al. (2009) Lemierre’s syndrome: A systematic review. Laryngoscope 119(8): 1552-1559.
- Dahlen G, Ebenfelt A (2011) Necrobacillosis in humans. Expert Rev Anti Infect Ther 9(2): 227-236.
- Riordan T (2007) Human infection with Fusobacterium necrophorum (Necrobacillosis), with a focus on Lemierre’s syndrome. Clin Microbiol Rev 20(4): 622-659.
- Jones JW, Riordan T, Morgan MS (2001) Investigation of postanginal sepsis and Lemierre’s syndrome in the South West Peninsula. Commun Dis Public Health 4(4): 278-281.
- Hagelskjaer Kristensen L, Prag J (2008) Localised Fusobacterium necrophorum infections: a prospective laboratory-based Danish study. Eur J Clin Microbiol Infect Dis 27(8): 733-739.
- Lemierre A (1936) On Certain Septicæmias Due to Anaerobic Organisms. Lancet 227(5874): 701-703.
- Dalen CT, Mekhail AM (2015) Lemierre syndrome: early recognition and management. CMAJ 187(16): 1229-1231.
- Rusan M, Klug TE, Ovesen T (2009) An overview of the microbiology of acute ear, nose and throat infections requiring hospitalisation. Eur J Clin Microbiol Infect Dis 28(3): 243-251.
