 Short Communication
Short CommunicationAbstract
This study aimed to analyze the safety reports of the organization of King Abdulaziz Medical City (KAMC); these safety reports included warfarin as a medication error or near-miss. The goal of this analysis is to optimize the reporting of incidents in the safety reporting system and to determine the factors contributing to errors in warfarin prescriptions. In this retrospective study, we used reports from 2013 to 2016 related to warfarin collected from the organization’s safety report system database. The data were extracted and analyzed to determine the number of yearly reports, contributing factors, and person-affected outcomes. Overall, 78 incidents were reported (2013: n=4, 2014: n=19, 2015: n=22, 2016: n=33); 73% of them did not reach the patient, and 26.9% did reach the patient. Of the 26.9% (n=21) that reached the patient, 16 did not cause harm, and only 5 of the patients needed monitoring to confirm a lack of harm.
There was a significant increase in warfarin-reported incidents over the years, which is an indication of an increased frequency of voluntary reporting in the system, along with a higher number of errors in warfarin prescriptions. The higher percentage of near-misses indicates a need to educate qualified healthcare providers, who are informed about fair culture and national and international safety standards for high-alert medication, about this issue. The organization implemented a new healthcare informatics system in 2015 and 2016; this new system was one of the important contributing factors, in addition to medication preparation errors and a lack of proper medication reconciliation.
Keywords: Warfarin; Medication Errors; Safety Reporting System
Short Communication
High-alert medications are not necessarily more common in medication errors; however, the mistakes in these medications heighten the risk of causing patients significant harm. Warfarin has been classified as a high-alert drug by the Institute for Safe Medication Practices [1]. Medication errors and adverse drug reactions are the main cause of harm among hospitalized patients [2]. One study reported that approximately 6.5 medication-related adverse events occurred per 100 hospitalizations and estimated that more than one-quarter of them are preventable causes of ADRs [3]. Medication errors are potentially preventable causes of ADRs that can occur at all stages of the medication process, e.g., prescription, transcription, dispensing, and administration [4]. Errors resulting in preventable ADEs frequently occur at the steps of ordering and administration but are less frequent in transcription and dispensing [3].
In one study, the authors compare preventable to nonpreventable events in terms of length of stay and cost. They found that potentially preventable ADEs doubled the total length of stay and health care costs [5]. Furthermore, anticoagulant medications, including warfarin, are among the most common medications that cause errors in the hospital setting [2,6]. Despite the implementation of electronic health records, including computerized provider order entry, medication errors, such as those involving anticoagulant medications, are common [7,8]. We chose warfarin in our study since the use of this medication has increased dramatically over the past several decades [9]. Moreover, according to U.S. Food and Drug Administration reporting system, warfarin is considered one of the top ten medications associated with serious adverse events such as bleeding [9]. The incidence of warfarin-related adverse drug events and person-affected outcomes have not yet been reported in our institution. This research aims to shed light on this subject.
The aim of this study is to analyze safety reports that included warfarin as a medication error or near-miss at King Abdulaziz Medical City (KAMC), National Guard Health Affairs, Central Region, to optimize the reporting of incidents in the safety reporting system and to determine the factors contributing to errors in warfarin prescriptions.
Methods
Design
Single-center retrospective cohort study.
Setting
The research was conducted in the King Abdulaziz Medical City-Riyadh Ministry of National Guard Health Affairs. The research was initiated in August 2017.
Data Source
In this study, we used reports from 2013 to 2016 related to warfarin that were collected from the organization’s safety report system database.
Research Instrument
The safety reporting system (SRS) refers to an electronic web-based tool utilized to report safety reports, collate related information and feedback. Reports to the SRS database are freetext fields with no minimum amount of information required to complete the report safety process. The contributing factors were described and analyzed using a fishbone diagram (Ishikawa).
Statistical Analysis
The data were extracted and described, and the analysis was performed to determine the number of yearly reports, contributing factors, and person-affected outcomes. Descriptive analyses were performed to determine the frequencies and characteristics of warfarin errors reported during the study period.
Results
A total of 78 adverse incidents were included in the study from 2013 to 2016 (Figure 1); 73% of them did not reach the patient, and 26.9% reached the patient. Out of the 26.9% (n=21), 16 did not cause harm, and only 5 of the patients needed monitoring to confirm no harm (Figure 2). The patient-affected outcomes are categorized alphabetically from A to I according to severity (Table 1) [10,11]. The analysis of the contributing factor was applied in the fishbone diagram for the incidents that reached the patients. Under the material factors, the IT/network problems were one of the main reasons for the incidents. In addition to personnel-related factors, other factors included a lack of quality control in the application of an independent double-check system for high-alert medications, miscommunication among staff and a lack of staff education. We also found that the workload and work environment had an impact on errors with respect to staffing deficiencies (Figure 3).
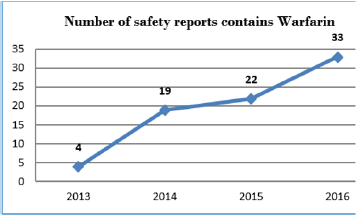
Figure 1: Number of Safety Reports Related to Warfarin.
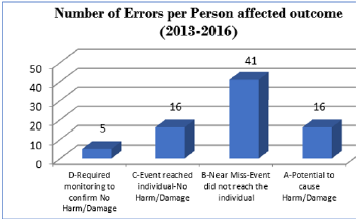
Figure 2: Number of Errors per Person affected outcome (2013-2016).
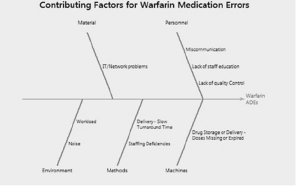
Figure 3: Factors contributing to warfarin medication errors.
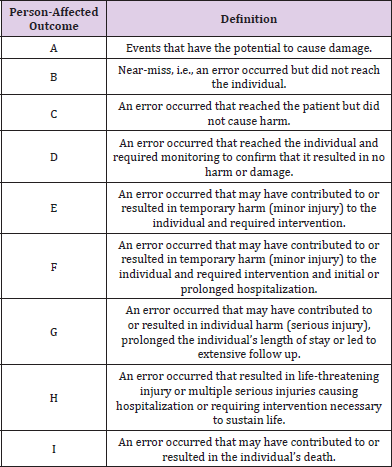
Table 1: Index for categorizing safety reports.
Limitations
The present study had some limitations. Like other voluntary reporting systems, the safety reporting system is inherently prone to underreporting. In addition, there is a lack of similar studies related to the reporting of medication errors, especially in the Middle East and for warfarin in particular.
Conclusion
There was an increase in warfarin-reported incidents throughout the years, which is an indication of an increased frequency of voluntary reports in the system, along with a higher number of errors in warfarin prescriptions. The higher percentage of near-misses indicates a need to educate qualified healthcare providers, who are informed about fair culture and national and international safety standards for high-alert medication, about this issue. The organization implemented a new healthcare informatics system in 2015 and 2016, which was one of the important factors contributing to medication errors, in addition to medication preparation errors and a lack of proper medication reconciliation.
Acknowledgement
This work was made possible by the generous cooperation of the pharmacists in the section of quality improvement.
Declaration of Interests
None declared.
Ethical Approval
This is a quality improvement project that was approved by the pharmacy department. The authors believe that no harm could result from this project to healthcare worker. Furthermore, this study does not reveal any confidential information or identifiers.
References
- (2018) ISMP List of High-Alert Medications in Acute Care Settings.
- Zaidenstein R, Eyal S, Efrati S, Akivison L, Koren Michowitz M, et al. (2002) Adverse drug events in hospitalized patients treated with cardiovascular drugs and anticoagulants. Pharmacoepidemiol Drug Saf 11(3): 235-238.
- Bates DW, Cullen DJ, Laird N, Petersen LA, Small SD, et al. (1995) Incidence of adverse drug events and potential adverse drug events. Implications for prevention. ADE Prevention Study Group. JAMA 274(1): 29-34.
- Poon EG, Keohane CA, Yoon CS, Ditmore M, Bane A, et al. (2010) Effect of bar-code technology on the safety of medication administration. J Med 362(18): 1698-1707.
- Bates DW, Spell N, Cullen DJ, Burdick E, Laird N, et al. (1997) The costs of adverse drug events in hospitalized patients. Adverse Drug Events Prevention Study Group. JAMA 277(4): 307-311.
- Classen DC, Jaser L, Budnitz DS (2010) Adverse drug events among hospitalized Medicare patients: epidemiology and national estimates from a new approach to surveillance. Jt Comm J Qual Patient Saf 36(1): 12-21.
- Grissinger MC, Hicks RW, Keroack MA, Marella WM, Vaida AJ (2010) Harmful medication errors involving unfractionated and low-molecular-weight heparin in three patient safety reporting programs. Jt Comm J Qual Patient Saf 36(5): 195-202.
- Fanikos J, Stapinski C, Koo S, Kucher N, Tsilimingras K, et al. (2004) Medication errors associated with anticoagulant therapy in the hospital. Am J Cardiol 94(4): 532-535.
- Wysowski DK, Nourjah P, Swartz L (2007) Bleeding complications with warfarin use: a prevalent adverse effect resulting in regulatory action. Archives of internal medicine 167(13): 1414-1419.
- Hartwig SC, Denger SD, Schneider PJ (1991) Severity-Indexed, Incident Report-Based Medication Error-Reporting Program. American Journal of Hospital Pharmacy 48(12): 2611-2616.
- (2001) National Coordinating Council for Medication Error Reporting and Prevention.
