 Review Article
Review ArticleABSTRACT
Purpose: Determine if hearing impairment impedes static and dynamic balance. Design: Three hundred subjects, 194 normal hearing (30.2 + 13.8 Yrs) and 106 (30.1 + 14.7 Yrs) hearing-impaired subjects, were administered a battery of 5 balance tests, 3 static and 2 dynamic tests.
Analysis: Mann-Whitney non-parametric and one-way ANOVA parametric tests were used to analyze the balance results comparisons between the two groups.
Results: Non-parametric Mann-Whitney results indicated significant superior static balance of the normal hearing group in both the dominant and non-dominant leg of the one-leg and stork static balance tests compared to the hearing-impaired group.
Keywords: Balance; Static and Dynamic Balance; Hearing Impairment; Vestibular Disorders
Introduction
Hearing impairment can be an inconvenience, an aggravation, or a public health hazard depending upon the extent of the problem. It is generally described as slight, mild, moderate, severe, or profound. It can be congenital (present at birth); or it can be acquired (occurred after birth). There are 4 types of hearing loss, conductive which are diseases or obstructions of the outer or middle ear; sensorineural which is damage to the delicate sensory hair of the inner ear or the nerves that supply it; a mix which is a combination of conductive and sensorineural; and central which is the result of damage or impairment to the nerves of the central nervous system [1]. Vestibular disorders are problems with parts of the inner ear and brain that process the sensory information involved with controlling balance and eye movements [2]. Hearing impairment may or may not be vestibular disorders. It could be related to conductive impairments or neuropathic, psychological, or idiopathic causes [3]. However, the most prevalent cause of acquired hearing impairment is the vestibular disorder, exposure to noise [4].
Childhood hearing impairment can pose significant public health problems associated with long- term academic and communication difficulties [5]. Therefore, identification of childhood hearing impairment is considered critical for normal speech, language, cognitive and social development [6]; however, routine screening does not generally include assessment of balance and motor deficits, even though some children demonstrate incoordination, clumsiness, and balance deficits that impede their optimal performance [7]. The ability to maintain postural stability or to control body movements is called balance. There are 2 types of balance, static and dynamic. Static balance is maintaining equilibrium when stationary, while dynamic balance is maintaining equilibrium when moving. Eyes, ears, physical conditioning, and proprioception are used to help sustain balance [8] and hearing impairment can impede balance and motor function [9,10]. The purpose of this study is to determine if hearing impairment significantly affects balance appraisal tests.
Design
Three hundred subjects (300), 173 males and 127 females, were administered a battery of 5 balance tests, 3 static tests and 2 dynamic tests. One hundred and six subjects (106), 64 males and 42 females, reported that they were hearing-impaired in some manner. See Table 1 for the subjects’ physical characteristics. The IRB approved study consisted of a convenience sample of 300 subjects. Prior to administering the battery of tests, the subjects were informed of the battery of tests that were to be performed, the description of the tests, and that the subjects could stop at any time during the tests. The subjects signed a consent form prior to the beginning of testing. The tests were conducted by University of New Orleans exercise physiology undergraduate students who were CITI-certified for Human Subjects Testing and trained to administer the battery of balance tests.

Table 1: Physical characteristics.
*- mean + standard deviation.
The battery of tests administered to the subjects consisted of the following tests. Brief descriptions of the tests are also included: [8, 11-15]
One-Leg Standing Balance Static Test (Right and Left Leg)
Stand on 1 leg without holding onto anything. Normal balance is one minute. Subjects scoring less than 30 seconds will need some work.
Stork Balance Static Test (Right and Left Leg)
Place the hands on the hips, position the non-supporting foot against the inside knee of the supporting leg. The subject raises the heel to balance on the ball of the foot. The stopwatch is started as the heel is raised from the floor. The stopwatch is stopped if the hand(s) come off the hips, the supporting foot swivels or moves (hops) in any direction, the non-supporting foot loses contact with the knee, or the heel of the supporting foot touches the floor. Average time is 25 - 39 seconds. Subjects scoring less than 10 seconds are considered to have poor static balance.
Timed Up-and-Go Dynamic Test
A chair is placed against a wall and a spot is measured and marked ten feet from the chair. The test is how long it takes to get up out of the chair, walk 10 feet, turn around, return to the chair and sit back down. If it takes the subject longer than 14 seconds, there is a high risk for falling.
The 5 Times Sit-to-Stand Dynamic Test
Sit in a chair. Whenever ready, stand up and down 5 complete times as fast as possible. Stand fully and sit down with the glutes touching the chair. Subjects without balance problems can do this test in less than 13 seconds.
The Balance Error Scoring System Static Test [16]
There are six positions of the balance error scoring system static test. Three stances (double-leg support, single-leg support, and tandem) are held for 20 seconds on two surfaces (firm floor and foam pad) for six permutations. During the tandem stance, the dominant foot is in front of the nondominant foot. During the single-leg stance, the subject stands on the nondominant foot. During the test, the eyes are closed and the hands are held on the hips (iliac crests).
Subjects are told to keep as steady as possible, and if they lose their balance, they are to try to regain the initial position as quickly as possible. Subjects are assessed one point for the following errors: lifting the hands off the iliac crests; opening the eyes; stepping, stumbling, or falling; remaining out of the test position for five seconds; moving the hip into more than 30° of hip flexion or abduction; or lifting the forefoot or heel. A trial is considered incomplete if the subject cannot hold the position without error for at least five seconds. The maximal number of errors per condition is 10. An incomplete condition is given the maximal number of points [10]. The numbers of errors for all six conditions are summed into a single score. For example, ages 20-39 years, mean + SD = 10.97 + 5.05 errors; 50-54 years, mean + SD = 12.73 + 6.07 errors; and 65- 69 years, mean + SD = 20.38 + 7.78 errors.
Limitations
Hearing impairments were self-reported by the participants. While completing preliminary anthropometric information, participants were asked if they were hearing-impaired. No additional questions were asked about the type or the degree of the hearing impairment.
Analysis
One-way analysis of variance (ANOVA) tests from the IBM Statistical Program for Social Sciences (SPSS) version 24 were used to compare the scores of the normal hearing subjects versus the scores of the impaired hearing subjects. One-way ANOVA was also used to compare the gender, age, height, and weight differences of the two groups. Levene’s tests were used to validate the comparisons of the data. The level of significance was set at 0.05. For the Levene tests to validate the One-way ANOVA comparison the significance of the Levene statistic should be greater than 0.05, indicating that the groups’ variances were not significantly different between each other. If the Levene tests validated the homogeneity of the variances of the gender groups, One-Way ANOVA parametric analysis were used. See Table 2 for results. The Mann-Whitney non-parametric tests were used to analyze the tests that were not validated by Levene’s homogeneity tests.
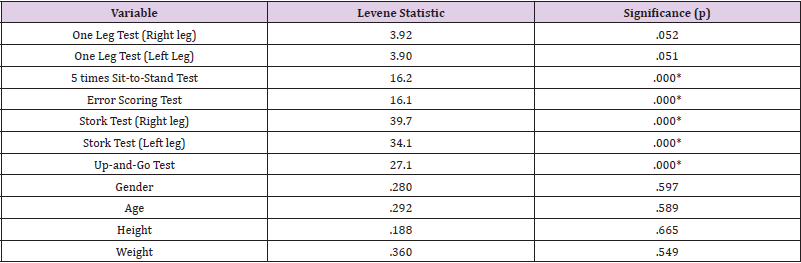
Table 2: Levene Test of Homogeneity.
*-Significant. Significance set at p < 0.05.; d.f. = (1, 298).
Results
Levene’s homogeneity tests validated the results of both the dominant and non-dominant one leg tests along with the gender, age, height, and weight of the 2 groups. Because the parametric oneway ANOVA results were not validated for the other 4 balance tests, non-parametric Mann-Whitney tests were applied to analyze the results of all 5 balance tests. One-way ANOVA results indicated no significant group differences regarding the gender, age, height, and weight of the participants. Both the dominant and non-dominant one-leg tests indicated significant differences between the groups with the normal hearing groups averaging 118.8 seconds versus 83.1 seconds for the hearing-impaired group for the right leg test [F (1,298) = 3.97, p < 0.05], and 113.7 seconds for the normal hearing group versus 77.9 seconds for the hearing-impaired group for the left leg test. [F (1,298) = 4.68, p < 0.05]. The non-parametric Mann- Whitney results indicated significant group differences in both the dominant and non-dominant one-leg and stork tests. See Table 3 for the results.
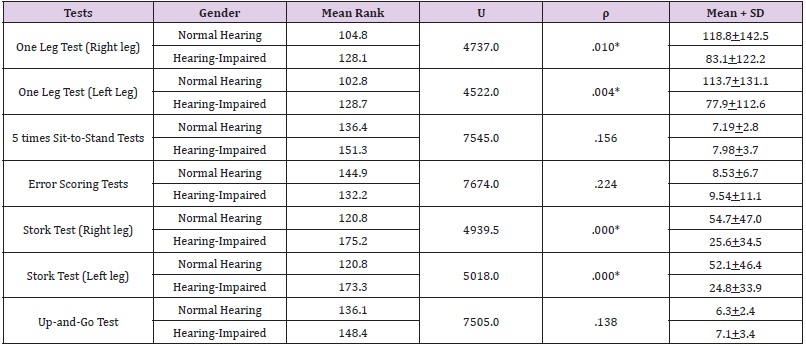
Table 3: Mann-Whitney Ranking Results.
*- Significant, Level of Significance ρ = 0.05.
Discussion
The study revealed that the hearing-impaired group scored significant deficient results in both the dominant and non-dominant legs in the one-leg static test and the stork static test. There were not significant group differences in the Error Scoring static test or in any of the dynamic balance tests. There were also no significant differences regarding the gender, age, height, or weight between the two groups that were analyzed. The question that first comes to mind is why the hearing-impaired group scored so poorly in the one-leg and stork static tests, but not in the Error-scoring static balance test. Review of the tests show that the one-leg and stork tests are solely unipedal static tests while the error scoring test is primarily a bipedal static test (4 tests are bipedal and 2 tests are unipedal) [17]. That would seem to indicate that the bipedal static stance in the test provides a more stable base to maintain static balance. Non-parametric analyses revealed no significant balance performance discrepancy between the two groups in the dynamic balance tests. This would seem to imply that while in motion other proprioception components compensate for the balance discrepancies of the hearing-impaired group that are distinguished when stationary.
An interesting aspect of the study was the high incidence of participants indicating they were hearing -impaired. The initial observation of the anthropometric data suggested that the data reported by the participants was suspect because of the high incidence of hearing impairment in a convenience sample There were 35.3% (106 out of 300) of the study participants that indicated they were hearing-impaired. That seems unusually high from a convenience sample population whose average age was 30.1+14.1 (mean + s.d.) years old; however, the comparative analyses indicating significant static balance differences between the 2 groups indicated that the reported anthropometric data was not suspect. The fact that there were no significant group differences regarding sex, age, height, and weight suggests that the group performance discrepancy was most likely attributed to the hearing-impaired group.
Conclusion
The study demonstrated that hearing impairment negatively impacts static balance and warrants the need for further investigation. The authors recommend additional testing to verify the results obtained from the study; and to secure larger samples that would include parametric analyses of all 5 balance tests used in the current study for a deeper insight into how balance impacts motor performance. Increasing the number of subjects in the convenience sample could improve the variances of the test groups, resulting in the Levene homogeneity test values validating the oneway ANOVA analyses for the balance test battery. The parametric one-way ANOVA test is a much more sensitive test than the nonparametric Mann-Whitney test.
The high incidence of subjects reporting hearing impairment is a concern and a possible indication of a public health problem. In future research additional anthropometric information could be gathered from the subject population to determine the type and extent of hearing impairment. The research could possibly identify the major cause of hearing impairment of the research subjects as an environmental one, such as the vestibular disorder of “exposure to noise.” If so, the environmental problem could be addressed by devising an action plan to reduce the high incidence of the environmental disorder [4].
Acknowledgements
The authors would like to thank the certified UNO exercise physiology majors who participated as testers in this motor learning balance study. No grant or outside funding was provided for this project.
References
- E Health MD (n.d.). Different types of hearing loss.
- Wiener-Vacher S (2008) Vestibular disorders in children. Intl J Audiology 47(9): 578-583.
- DeKegel A, Maes L, Baetens T, Van Waelvelde (2012) The influence of a vestibular dysfunction on the motor development of hearing-impaired children. Laryngoscope 122(12): 2837-2843.
- (2007) The Merck Manual’s Online Medical Library. Hearing loss and deafness.
- Davis A (1997) Epidemiology of hearing impairment. Otolaryngology 1997 6th (Edn). Oxford 4: 18-19.
- Windmill I (1998) Universal screening of infants for hearing loss: Further justification J Pediatr pp. 318-319.
- Butterfield S (1986) Gross motor profiles of deaf children. Percept Mot Skills 62(1): 68-70.
- Miller T (2012) NSCA’s guide to tests and assessments. Champaign, IL: Human Kinetics.
- Rajendran V, Roy F, Jeevanantham D (2012) Postural control, motor skills, and health-related quality of life in children with hearing impairment: A systematic review. Eur Arch Otorhinolaryngol 269: 1063-1071.
- Rajendran V, Roy F (2011) An overview of motor skill performance and balance in hearing impaired children. Ital J Pediatr 37(1): 33.
- Collen F, Wade D, Bradshaw C (1990) Mobility after stroke; reliability of measures of impairment and disability. Int Disabil Stud 12(1): 6-9.
- Riemann B, Guskiewicz K, Shields E (1998) Relationship between clinical and force plate measures of postural stability. Sport Rehabilitation 8(2): 71-82.
- Goldie P, Matyas T, Spencer K, McGinley R (1990) Postural control in standing following stroke; test-retest reliability of some quantitative clinical tests. Phys Ther 70(4): 234-243.
- Bohannon R, Larkin P, Cook A, Gear J, Singer J (1984) Decrease in Timed Balance Test Scores with Aging. Physical Therapy 64(7): 1067- 1070.
- Giorgetti M, Harris B, Jette A (1998) Reliability of clinical balance outcome measures in the elderly. Physiother Res Int 3(4): 274-283.
- Iverson G, Kaarto M, Koehle M (2008) Normative data for the balance error scoring system:Implications for brain injury evaluation. Brain Injury pp. 147-152.
- Bonis M, Tillery K (2021) Do collegiate athletes display better balance skills than their non-athlete counterparts? Biomed J Sci & Tech Res 34(4).
