 Case Report
Case ReportAbstract
Conduction disturbances complicating acute myocardial infarction with persistent ST segment elevation are common, especially those of high degree in previous myocardial infarctions. Do these complications occur in the acute phase, before revascularization, with a poor prognosis immediately justifying myocardial reperfusion as well as the placement of an electro systolic training lead. However, their absence before revascularization to occur in post percutaneous reperfusion by angioplasty with placement of an active stent on the culprit artery, with an increase in the ST elevation, is unprecedented and raises as many questions as possible whereas the Stent in place remains permeable. We report the case of a patient presenting, initially, a 3rd degree atrioventricular block after percutaneous revascularization of an ST + extended anteriorly by angioplasty and placement of an active stent on the anterior interventricular coronary artery permeable after a second post-critical coronary angiography.
Keywords: Anterior Myocardial Infarction; 3rd Degree Atrioventricular Block; Cardiac Arrest; Anterior Interventricular Artery; Electro systolic Training Lead; Fibrinolysis; Coronary Vasospasm
Introduction
Complete or third degree atrioventricular block (cAVB), defined by the complete and permanent interruption of the transmission of atrial impulses to the ventricles [1,2] is one of the early and relatively frequent complications of myocardial necrosis whose pathophysiology and the course differs depending on the seat of the infarction; indeed, AVB always shows anatomically extensive infarcts, the mortality of which from previous infarctions complicated by AVB remains considerable (> 60%) in the absence of early revascularization [3,4]. This complication, very common before the era of revascularization, occurs in the acute phase. Their early installation in post reperfusion of an extensive anterior myocardial infarction is unprecedented and has a particular aspect which justifies our review. We report a case of complete atrioventricular block occurring initially after Percutaneous Revascularization (PR) of extensive anterior ST + (STEMI-EA).
Clinical Case
This is a 51-year-old patient, chronic active smoker and diabetic discovered in hospital, with no history; he presented with an inaugural retrosternal infarction stabbing chest pain, radiating to the upper left limbs for which he consulted at H9 in the Emergency Department of the Ibn Sina University Hospital. On clinical examination, the eupneic patient was unwell with a good hemodynamic state, as for his electrocardiogram at H9, we note a super shift of the ST segment in the extended anterior (Figures 1), from which he benefited from thrombolysis with success criteria, and the next day
a) A biological balance made of troponin> 50,000 ng / ml, potassium at 5mmol / l of a DFG at 66 ml / min / 1.73m2.
b) A trans thoracic Doppler echocardiography which shows lesions of disturbed kinetics.
c) A coronary angiogram showing a sub-occluded lesion of the average anterior interventricular artery (AIV) having undergone angioplasty and placement of an active stent.
The immediate evolution, 2 hours later, was marked by the inaugural onset of a complete AVB and a cardiac arrest by asystole, recovered by resuscitation measure, followed by 4 episodes of cardiac pause with an increase in the elevation of the ST segment in the same territory (Figures 2).
d) He underwent a second coronary angiography showing an active stent in place and permeable, without other culpable lesions.
e) Then the setting of a provisional electro systolic training lead.
The medical consequences are marked by a spontaneous recovery after 48 hours of return to sinus rhythm. The patient is declared discharged, the course of which is marked by the sudden onset of cardiac arrest at home after 3 weeks.
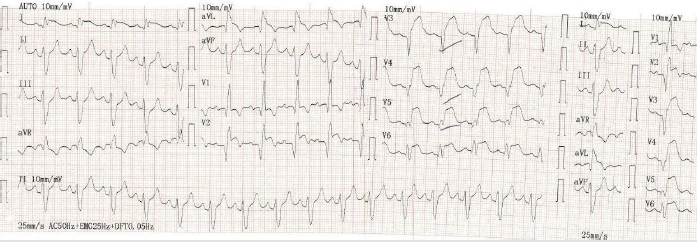
Figure 1: Patient admitted for infarctoid chest pain to Avicenna’s Emergency Department, at H8, related to an extensive anterior ST + thrombolysed with successful Metalysis at H9: pain sedation and regression of ST + amplitude. And his troponin was> 50,000 ng / ml.
Note: Day 1: ST segment shift in extended anterior before thrombolysis, before percutaneous coronary revascularization.
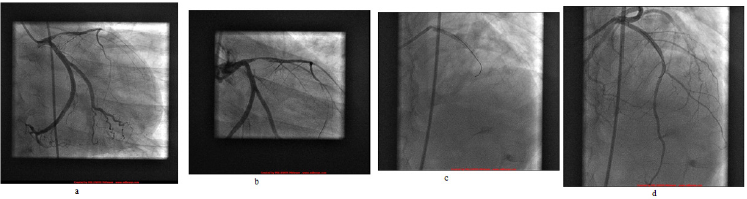
Figure 2:
a. Figure b: Coronary angiography image 1: sub-occlusion of the proximal anterior interventricular artery and
b. Figure d: Coronary angiography image 2: Active permeable stent in place on the proximal anterior interventriventricular artery.
Note: Day 2: the next day, he was transferred to Cardiology B, where he received an ETT, followed by a coronary angiography at 1:30 p.m. Objectifying a sub-occluded proximal VIA. He was then transferred to the Intensive Care Unit of Cardiology B at 2:50 p.m.
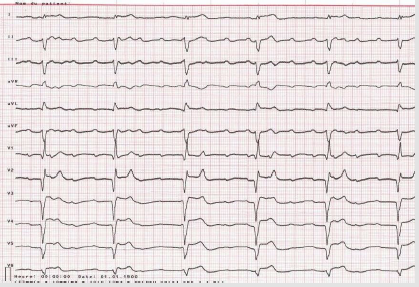
Figure 3: Inaugural complete AVB occurring 2 hours after coronary angiography revascularization.
Note: Day 2: At 4 p.m., the patient under medical scope switches to complete AVB.
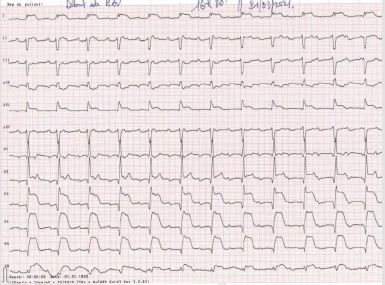
Figure 4: Inaugural full AVB with increased ST segment elevation post-revascularization, 3 hours after coronary angiography.
Note: 6h, then he modifies his extended anterior ST + segment by increasing amplitude during his complete AVB with clinically hemodynamic instability and altered consciousness.
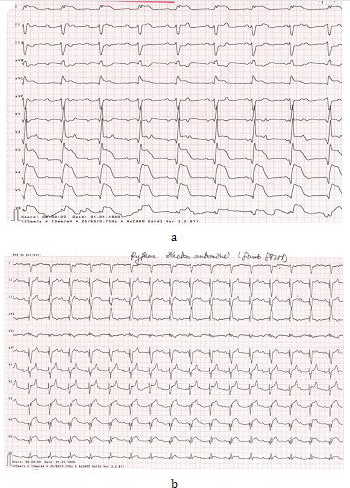
Figure 5:
a. Post cardiac arrest recovered, persistence of complete AVB with shifting of the ST segment, 3 hours after coronary angiography.
b. Electro rhythm trained by the Electro-systolic Training Probe probe.
Note: 5:00 p.m., cardiac arrest from asystole ensues requiring resuscitation by cardio thoracic massage for 10 to 15 minutes with the use of adrenaline and other drugs. The patient is then taken to the Catheterization room for a second coronary angiography by the same day team. Second coronary angiography showing a stent in place, permeable with good TIMI 3. Then installation of an Electro-systolic Training Probe by the Rhythmology team.
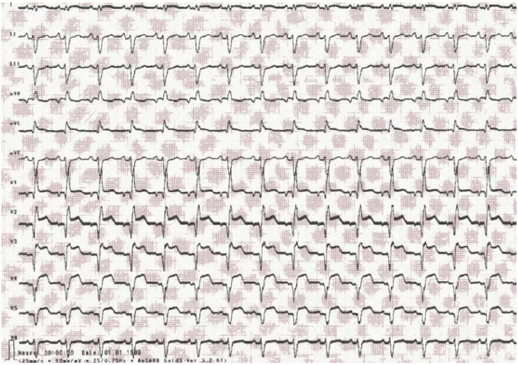
Figure 6: Return to sinus rhythm after 48 h, with good clinical and hemodynamic and rhythmic evolution. Note: Day 5: Return to sinus rhythm before discharge from the hospital.
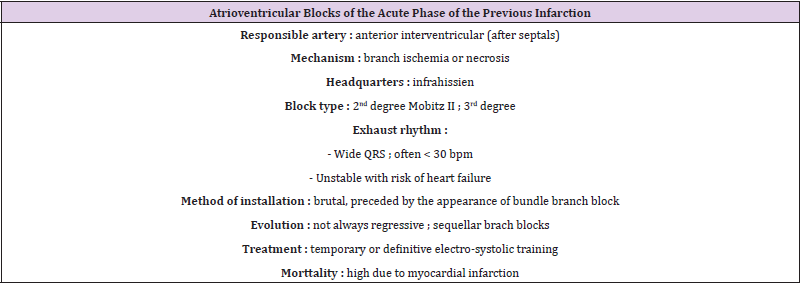
Table 1:
References
- Pierre Taboulet (2018) ECG de A à Edition 2018, Maloine.
- Pierre Taboulet (2014) Blocs sinoauriculaires et auriculoventriculaires. Urgences SFMU.
- A Leenhardt, C Sebag, F Extramiana, V Algalarrondo (2012) L Essentiel en RYTHMOLOGIE. In: A Leenhardt, C Sebag, F Extramiana, V Algalarrondo (Eds.)., Lavoisier SAS, France.
- Jesse J Corry, Andrew M Naidech (2013) Cardiovascular Monitoring and Complications. Neurocritical Care Society Practice Update
- C Latremouille, F Lintz (2005) Anatomie du cœur. Elsevier Masson.
- UJ Ortved Gang, A Hvelplund (2012) High-degree atrioventricular block complicating ST-segment elevation myocardial infarction in the era of primary percutaneous coronary intervention. ESC 14(11): 1639-1664.
- Hymie H, Chera Cristina A, Mitre Justin Nealis, Alex Mironov Adam, S Budzikowski (2018) Frequency of Complete Atrioventricular Block Complicating ST-Elevation Myocardial Infarction in a Patient Undergoing Primary Percutaneous Coronary Intervention. Cardiology 140(3): 146-151.
- Harpaz D, Behar S, Gottlieb S, Boyko V, Kishon Y (1999) Complete atrioventricular block complicating acute myocardial infarction in the thrombolytic era. SPRINT Study Group and the Israeli Thrombolytic Survey Group. Secondary Prevention Reinfarction Israeli Nifedipine Trial. J Am Coll Cardiol 34(6): 1721-1728.
- Hoa L Nguyen, Darleen Lessard (2008) Thirty-year trends (1975-2005) in the magnitude and hospital death rates associated with complete heart block in patients with acute myocardial infarction: A population-based perspective. American Heart Journal August 156(2): 227-233.
- Chloé Physiologie del’hémostase. MCU-PH, Laboratoire d’hématologie, Hôpital Haut Levêque.
- JY Artigou, JJ Monsuez (2020) Cardiologie et Maladies Vasculaires. Société Française de Cardiologie. Offre premium. In: JY Artigou, JJ Monsuez (Eds.)., (2020th)., Elsevier, USA.
- Kardasz I, De Caterina R (2007) Myocardial infarction with normal coronary arteries:a conundrum with multiple aetiologies and variable prognosis: an update. JIntern Med 261(4): 330-348.
- Lanza GA, Careri G, Crea F (2011) Mechanisms of coronary artery spasm. Circulation 124(16): 1774-1782.
- Takagi Y (2013) Prognostic stratification of patients with vasospastic angina: a comprehensive clinical risk score developed by the Japanese Coronary Spasm Association. J Am Coll Cardiol 62(13): 1144-1153.
- Beltrame JF (2016) The who, what, why, when, how and where of vasospasticangina. Circ J 80(2): 289-298.
- Benamer H (2019) Langor spastique : une pathologie sous-diagnostiqué Ann Cardiol Angeiol (Paris). 68(5).
- Picard F (2019) Vasospastic angina: A literature review of current evidence. Arch Cardiovasc Dis 112(1): 44-55.
- D Attias, N Lellouche (2018) Cardiologie vasculaire. In: D Attias, N Lellouche (Eds.)., (8th)., Cardiologie.
- Borja Ibanez, Stefan James (2018) Guidelines for the management of acute myocardial infarction in patients presenting xith ST-segment elevation. 2017 ESC; EHJ 39: 119-177.
