 Research Article
Research ArticleABSTRACT
In this study, a model eye was created with a film camera, fitted with a manual focus 50mm lens. Then, in order to simulate the LASIK ablation of a -2.00 myope, a +2.00-converging spherical lens with a 5mm hole in its optical center was placed over the main lens. Photographs were then taken of a static object and contrast sensitivity measurements were obtained with a CSV-1000 Vector Vision tester at 6-cycles/degree for lens apertures F/4 through F/16. Using geometrical optics, the images recorded on these photographs showed that spherical aberrations are produced at large apertures, F/8 or greater, while small lens apertures, F/11 through F16, did not produce spherical aberrations. The overall findings of the study indicate that for large apertures within the model eye, there is a decrease in contrast sensitivity and image quality after the simulated LASIK ablation was performed on the camera lens. Since both the model eye used in this study and the human eye form images via the refraction of light in the same way the hope is that this form of sample photography would allow patients to preview what their vision will be after their LASIK surgery. This would be possible by examining test photographs taken with an ablated lens; a lens constructed using an individualized ablation algorithm for a specific patient (as opposed to the standard simulated ablation used in this study). The image quality of these test photographs would reflect the deleterious effects of spherical aberrations in a way that is analogous to the quality of the patient’s potentially rehabilitated vision after LASIK. After carefully reviewing the test photographs the patient could better understand how their vision would be impacted and decide if LASIK is right for them. The eye surgeon performing the procedure would also be protected because it would help prevent unrealistic expectations on behalf of the patient. In addition, because these photographs show the actual image quality, contrast sensitivity measurements are no longer needed for evaluating LASIK. The validity of this theory would need to be confirmed with a clinical study.
Introduction
Model eyes and devices that generate controlled amounts of spherical aberrations, have many optical applications. Fernandez and Artal proposed a model eye that allowed precise control of aberrations that could be used to test and evaluate adaptive optics instruments for ophthalmic applications. Their model eye used a meniscus lens together with a modal crystal lens and a diffuser that acted as a retina [1]. Buchroeder developed an aberration generator that was used to study the effects of aberrations on image quality [2]. Palusinski constructed a device that produced aberrations by laterally shifting a pair of concentric plates relative to each other to produce aberrations. This device has applications in aberration control of lens systems [3].
As noted above model eyes are useful to study optical aberrations. In the study that was conducted for the purposes of this paper the same approach was used to document the optical properties of a model eye, consisting of a film camera and a manual focus 50mm lens, that undergoes simulated LASIK ablation. To simulate the LASIK ablation of a -2.00 myope a +2.00 lens with a 5mm hole in the optical center is placed over the 50mm lens. Contrast sensitivity measurements of the model eye were obtained using a CSV-1000 Vector Vision tester at 6-cycles/degree. Following the same methodology [1-3] photographs are taken of a static object for various lens apertures. Using geometrical optics, it is shown that spherical. aberrations are generated in the model eye after simulated LASIK ablation for certain values of lens aperture. The detrimental effect of these aberrations on image quality is determined with the CSV-1000 and the photographs of a static object. Loss of contrast sensitivity after LASIK is a common problem that has been analyzed in other studies [4,5]. However, in this study the results of the CSV-1000 are compared with the photographs of a static object in order to determine which is more useful in analyzing image quality after LASIK.
The model eye described herein provides a direct methodology to evaluate the image quality for a specific type of simulated LASIK ablation (a +2.00 lens with a 5mm hole in the optical center). The analysis presented in this study suggests that the model eye could also be used with a LASIK ablation of a more advanced design. For example, instead of using a +2.00 lens with a hole in the optical center to simulate LASIK ablation the actual ablation algorithm of patient could be used. Photographs of a static object with this ablation algorithm would have a similar image quality as the patient after their LASIK surgery. This would provide the patient with a preview of their vision prior to having LASIK.
The Model
Diagram 1 is a schematic diagram of the model eye, consisting of a film camera and a manual focus 50mm lens, when light rays from a distant object focus sharply on the film plane at E. A +2.00-converging lens is mounted on the 50mm lens by using the mounting ring from a UV filter. The +2.00-converging lens moves the focal point from point E to M in front of the film plane as shown in Diagram 2. Thus, the +2.00-converging lens would produce a sharp image at M and a blurred image on the film plane just as if the model eye had myopia. LASIK ablation is simulated in the model eye by drilling a hole in the optical center of the +2.00-converging lens. Diagram 3 shows that depending on the optical path the light rays take the model eye has two different focal points at E and M. Light rays that pass through the hole have a focal point at E. Those that pass through the circular area surrounding the hole are subjected to a greater refractive power and have a focal point at M. By definition spherical aberrations are produced by a lens when light rays from the periphery are subjected to a greater refractive power than those closer to the axis [6]. It follows that for every axial object point there will be an axial image that is a “blur circle” instead of a point and nowhere will the image be sharp [7]. The sharpest image is where the cross section of the beam of light is smallest and is called the circle of least confusion. The location of the circle of least confusion in the model eye is between focal points E and M. Geometrical optics predicts that the central area of a photograph taken with the model eye will be blurred when there are two focal points E and M.
From the above discussion it follows that the lens aperture can be used to eliminate spherical aberrations in the model eye. When the aperture is F/16 or F/11 the lens diaphragm is small enough (see Table 1) to block the peripheral light rays and an axial image is produced only by the light rays that pass through the hole and converge at their focal point E. For this case every axial object point will have an axial image point and the model eye will have a sharp image at the film plane E. Hence there is no spherical aberration, and the image quality is good. However, for F/8 and larger apertures light rays from the circular area surrounding the hole will also enter the model eye producing focal points at E and M. As explained above this results in spherical aberrations.
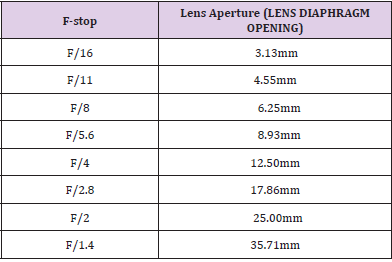
Table 1:
Measurements
A Pentax Spotmatic camera body and a Takumar manual focus 50mm lens is used as the model eye. A +2.00-converging lens with a 5mm hole in its optical center is mounted on the 50mm lens by using the mounting ring from a UV filter to simulate LASIK ablation. The contrast sensitivity of the model eye is measured with a CSV-1000 Vector Vision tester at 6-cycles/degree. Patients with cataracts are also tested to determine their glare disability at 6-cycles/degree. The experimental set up for measuring the contrast sensitivity for apertures F/16 through F/4 is as follows. The model eye was mounted on a simple tripod eight feet from the CSV-1000 tester. The model eye and ROW B (6 cycles/degree) of the CSV-1000 tester are set at the same height. After the camera is focused on row B of the CSV-1000 a photograph is taken at F/16. Then the +2.00 lens with a hole is carefully mounted on the 50mm lens so as not to alter the focus and a photograph is also taken at F/16. This process is repeated for apertures F/11, F/8, F/5.6 and F/4. Kodak Tri-X film was used to take the photographs. The photographic film that was obtained using the CSV-1000 as described above was manually examined with a Rodagon 50mm lens using forward illumination (the bulb was behind the photographic film) with a 14-watt bulb to determine where the patterns cannot be resolved. The results obtained for the contrast sensitivity are given in Table 2. Using the same tripod and film the model eye was used to take photographs of the authors favorite car for apertures F/4 to F/16 with and without the +2.00 lens with a hole.
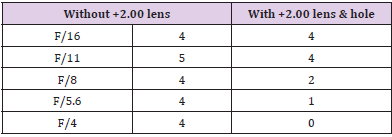
Table 2:
Discussion
The study described herein used a CSV-1000 and photographs of a static object taken with a “model eye” in order to demonstrate the effect of altered aperture size on central image quality and contrast sensitivity. Specifically, for apertures F/8 and larger, spherical aberrations were produced which reduced the central image quality of a static object as shown in Figures 1,2, 4 & 6, respectively. For each ascending aperture size, the effects of the spherical aberrations on the central image quality can be clearly seen by comparing Figure 2 with 1, Figure 4 with 3 and Figure 6 with 5 (note that Figures 1,3,5 do not have spherical aberrations induced by simulated LASIK ablation). When the lens aperture is small enough, at F/11 and F/16, light from the circular area surrounding the hole is blocked and no spherical aberrations are produced, and thus the central image quality remains essentially unchanged. This is made evident by comparing the central images in Figure 7 with 8 and Figure 9 with 10.
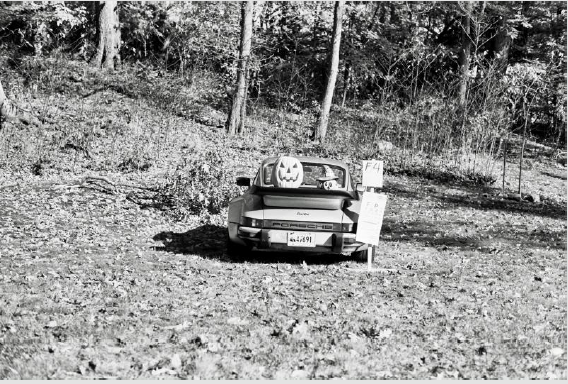
Figure 1: Figure 1 is a photograph taken with the model eye at F/4 without simulated LASIK ablation. It has uniformly good resolution and contrast. The corresponding contrast sensitivity measurement is 4.

Figure 2: The photograph in Figure 2 was taken with the model eye at F/4 with simulated LASIK ablation. The measured contrast sensitivity is 0. Note that all detail is lost in the center and only the general shape of the central object remains.
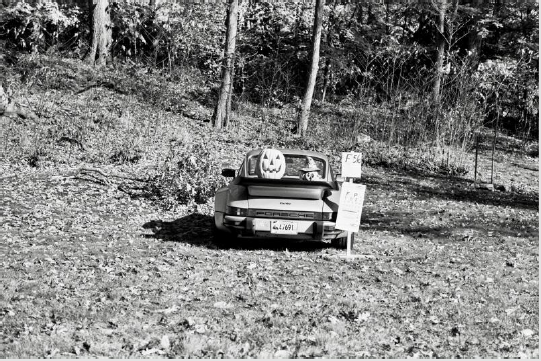
Figure 3: Figure 3 is a photograph with the model eye at F/5.6 without simulated LASIK ablation. It has good contrast and sensitivity. The corresponding contrast sensitivity measurement is 4.

Figure 4: Figure 4 is a photograph taken with the model eye at F/5.6 with simulated LASIK ablation. The corresponding contrast sensitivity measurement is 1. Note The central image quality of the central object is poor but improved from Figure 2.

Figure 5: Figure 5 is a photograph taken with the model eye at F/8 without simulated LASIK ablation. The contrast and resolution of this photograph is good. The corresponding contrast sensitivity measurement is 4.

Figure 6: Figure 6 is a photograph with the model eye at F/8 with simulated LASIK ablation. The corresponding contrast sensitivity measurement is 2 and the central image quality has improved enough to make the letters of the license plate almost distinguishable.
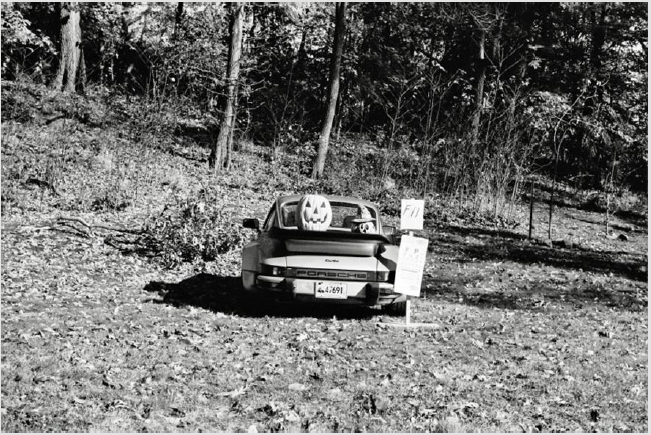
Figure 7: Figure 7 is a photograph with the model eye at F/11 without simulated LASIK ablation. The image quality is good, and the corresponding contrast sensitivity measurement is 5.
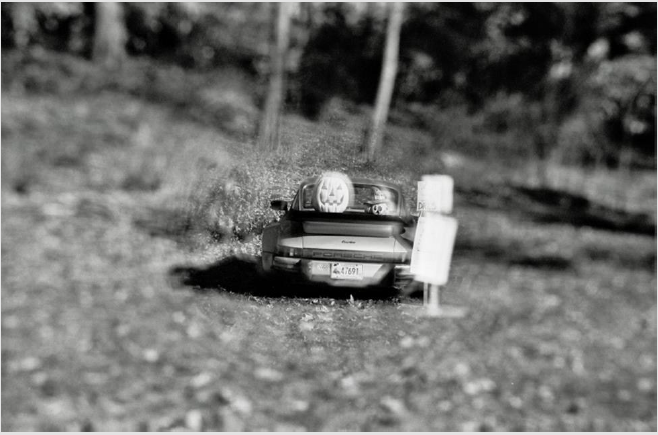
Figure 8: Figure 8 shows the model eye at F/11 with simulated LASIK ablation. The corresponding contrast sensitivity measurement is 4 and the central image quality is good.
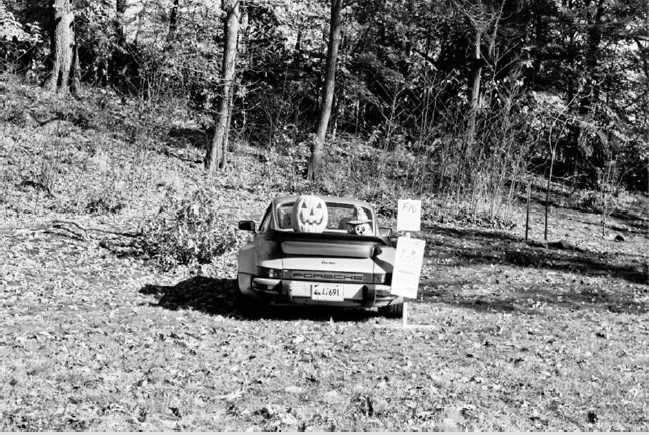
Figure 9: Figure 9 is a photograph with the model eye at F/16 without simulated LASIK ablation the +2.00. The image quality is good, and the corresponding contrast sensitivity measurement is 4.

Figure 10: Figure 10 is a photograph with the model eye at F/16 with simulated LASIK ablation. The central image quality is very good, and the corresponding contrast sensitivity measurement is 4.
Contrast sensitivity measurements for the model eye as a function of aperture are provided in Table 2. These measurements illustrate that when the apertures were restricted to small values in the model eye after simulated LASIK ablation did not produce spherical aberrations, the contrast sensitivity is on par with the model eye when it did not undergo simulated LASIK ablation. For large apertures, F/8 or larger, spherical aberrations were produced after simulated LASIK ablation that lowered the contrast sensitivity. As the aperture increases so does the number of spherical aberrations that are produced. At F/4 the number of spherical aberrations produced in the model eye after simulated LASIK ablation are so great that the contrast sensitivity is zero. The details of an object with a contrast sensitivity of zero are unrecognizable. This prediction is confirmed in Figure 2.
The simulated LASIK ablation of the model eye was accomplished by drilling a 5mm hole in the optical center of the +2.00-converging lens. This hole defined the ablation zone of the +2.00 lens. When light passed through the ablation zone, it would focus on the film plane. The light that passed through the outside of the ablation zone was subjected to a greater refractive power, which caused it to focus in front of the film plane, as opposed to on it. Figure 3. Spherical aberrations were produced when light rays from outside the ablation zone joined those from within the ablation zone. When this occurred, the best image was at the circle of least confusion, which in the model eye was located in front of the film plane. As the lens aperture was increased, lighter from outside the ablation zone entered the model eye and thus moved the location of the circle of least confusion further away from the film plane. This is why the image quality of the model eye deteriorated when the lens aperture was increased. Conversely, decreasing the lens aperture reduced the amount of light that entered the model eye from outside the ablation zone. Thus, the amount of spherical aberration was reduced, and the circle of least confusion moved closer to the film plane. This is why the image quality improves when the lens aperture was decreased. The best image quality occurred. when the lens aperture was small enough to block out all the light from outside the ablation zone. In this instance, the circle of least confusion moved to the film plane and shrunk to a point.
Because the same refraction laws apply in principle to image formation in the model eye as they would to the human eye, the above discussion also applies to the LASIK ablation of a human cornea. The simulated ablation in the model eye was represented by a 5mm hole in the optical center of a +2.00 lens. In order to correct the refractive error of a patient with LASIK the cornea is ablated according to a proprietary algorithm. It was shown in the model eye that the amount of spherical aberration is determined by the magnitude of the lens aperture. This would also be true for an eye after LASIK surgery, except that instead of discussing ablation in terms of lens aperture, it would be in terms of pupil size. Just like with the model eye used in this study, a sufficiently small pupil in a patient would eliminate spherical aberrations and result in excellent vision post-surgery. However, when the pupil size increases sufficiently, spherical aberrations are produced that would cause the patient to experience reduced contrast sensitivity and image quality. Decreased contrast sensitivity is a very common problem after LASIK and is why many patients have trouble driving at night [5]. These problems occur because the size of the pupil increases in the dark and as explained in this study, the enlarged pupil results in spherical aberrations. In the model eye described in this study a 5mm hole was drilled in the +2.00 lens in order to simulate LASIK ablation of a -2.00 myope. However, if this hole was replaced by the ablation algorithm of a specific patient with -2.00 myopia, what would the photographs taken with this model eye show? Theoretically these photographs would show the same image quality that the patient would have after their LASIK surgery. In turn, these photographs would allow a patient to preview the quality of their vision, prior to actually having the LASIK procedure. Below are outlined the steps for previewing the LASIK surgery.
1) The patient gets a full ophthalmologic evaluation to determine if he is a candidate for LASIK. This will include measuring corneal thickness, topography and refractive error. So far nothing is different from what is usually done. Normally the next step is for the patient to make an appointment to have the surgery and the laser ablates the cornea according to a proprietary algorithm (it is a function of corneal thickness and topography, refractive error and possibly something else).
2) The refractive error information is used to make the RElens. The RE-lens is similar to the +2.00 lens that is used in this paper and is fitted in the same way to the front of the main lens of the model eye. The RE-lens is shaped from a blank by a computer-controlled lens grinding machine (this technology is also used to make progressive lenses for glasses).
3) The anterior surface of the RE-lens is reshaped, using the same lens grinding machine, to mimic the LASIK ablation of the patient. If the ablation algorithm that is going to be used on the patient is available (that is the best choice) it would be used to reshape the anterior surface of the RE-lens (call it REs-lens after reshaping). If the algorithm is not available, it would have to be estimated.
4) Once the REs-lens is ready it is fitted to the model eye and used to take photographs of a set of predetermined static objects using various aperture sizes of the main lens of the model eye. The best static objects for this purpose may require a clinical test.
5) The patient is brought back to the office and shown the photographs of the static objects taken with the model eye using the REs-lens that was created from their optical information. These photographs would allow the patient to preview the quality of their vision, prior to actually having the LASIK procedure.
6) The results of the photographs are carefully explained especially when a potential for poor image quality exists, and a copy is given to the patient. The next step is for the patient to decide what he wants to do. After the vision preview the patient is armed with better information than they are presently and could better determine if LASIK is the right choice for them. The vision preview would also benefit the surgeon because it would help avoid unrealistic expectations about vision improvement on behalf of the patient. In addition, because these photographs show the actual image quality, contrast sensitivity measurements are no longer needed for evaluating LASIK. The results described above would first have to be verified and optimized with a clinical study. This is especially important in designing the RE-s lens so that it mimics the LASIK ablation precisely.
Conflict of Interest
The authors declare that there is no conflict of interest.
References
- Enrique Fernandez, Pablo Artal (2007) Dynamic Model Eye for Adaptive Optics Testing.Journal of Applied Optics46 (28): 6971-6977.
- Buchroeder, Richard, Hooker (1975) Aberration Generator. Journal of Applied Optics 14(10): 2476-2479.
- Palusinski, Iwona Lateral Shift (1999) Variable Aberration Generator. Journal of Applied Optics 38: 86-90.
- Holladay JT, A Lang V Portney (1999) Analysis of edge glare phenomena in intraocular lens edge designs. Journal of Cataract and Refractive Surgery 25(6):748-752.
- Nayori Yamane, Kazunori Miyata, Tomokazu Samejima, Takahiro Hiraoka, Takahiro Kiuchi, et al. (2004) Ocular higher-order aberrations and contrast sensitivity after conventional laser in situ keratomileusis. Investigative Ophthalmology, Vis Scii 45(11): 3986-3990.
- Sears and Zemansky: University Physics, 2nd (edn.). 3: 776.
- Optics for Clinicians :2nd (edn.). pp. 283.
