 Research Article
Research ArticleAbstract
The work is compiled from preclinical studies on volunteers, with the assistance of consultants from dental clinics. It is shown that the topic of preventive and preclinical (extra-clinical) dental care has not been developed (despite the progress in practical prosthetic and filling dentistry).
a) In the introduction, the rationale for the need for such work is presented, with an emphasis on the natural basis of the processes of self-restoration of teeth. The authors draw broad analogies with self-restoration in technical (construction, road, auto, air), medical (self-medication / prevention of suppuration and small scratches), and other areas.
b) Theoretical assumptions and views on the processes of self-restoration of carious, traumatic and other dental lesions are presented. Methods for creating tooth powders from public&cheap components are proposed for use by non-specialists in places unsuitable for traditional treatment & prophylaxis.
c) All these assumptions and hypotheses were confirmed in the results of observations as the well-being of patients as with visual information (photo, X-ray images) of the treated groups of affected teeth.
d) The conclusions made confirm the possibility of effective prophylaxis and selfrestoration of dental systems by non-operational exposure to special complexes of dental powders, pastes and rinsing systems (in compliance with the correct teeth’s exploitation).
Introduction and Substantiation of the Topic
Prevention of dental diseases should become the main direction of development of modern dentistry.
Dental Wear and Caries
Dental wear and caries are not necessarily a harmful acquisition of civilization. Teeth work at the forefront of life in extreme conditions, withstanding colossal changes in temperature, aggressive influences and pressures. In fact, they work in roughly the same conditions as abrasive cutting edges, car tires, shoe soles and other wear&tear parts. In evolution period when the human body was formed by Nature, only two changes of teeth (milk and permanent) were enough - for in prehistoric times a person lived ≤30+-10 years (as other big animals). Also, the teeth (as said Russian writer-doctor Veresaev [1]) were adapted for completely other loads. They were perfectly suited for chewing materials of medium hardness at moderate temperatures [1]. But now teeth often process food that is too soft or too hard, very sweet, salty or too sour, often with a sharp change from cold to too hot. But this requires completely different teeth, which are not able to appear in just 5-10 thousand years of evolution [1]. Thus, wear and tear of teeth in our conditions is a normal phenomenon (especially after 40 years), and Dentistry has become an adequate response to this problem in recent centuries. De-facto we able now change our teeth many times (as crocodiles etc.).
Prehistory
The issues of caries prevention and treatment have been seriously studied for last 150-200 years, and in 20th century we can talk about reaching a new level. But in the post-war period (since 1950s), practical dentistry made a real breakthrough. Really, Dentistry (like most sciences) has made a colossal step forward over the past 100, and even 30 years. For example, 150- 200 years ago, a dentist was called, at best, a “healer-zodder”; in the usual case, his functions were performed by healers or ... a barber (hairdressers)! The qualificate dentists were at best, near royal or wery-rich persons. As a rule, all people simply engaged in more or less successful self-medication. But already 150 years ago, the first filling compounds appeared based on rubber, mixtures of tar and natural resins with cements [2].
Methods and even materials of 100 years ago (cements, “Bowen-s resin” [2]) are already similar to modern ones. Post-war dentistry of the 50-70s is very similar to modern dentistry. We are well aware of the state of the art. Nevertheless, the issues of prevention and self-healing of carious diseases remain in poorly studied topics. They are on the sidelines of the main dentalbusiness, which operates 85% in the field of prosthetics, plombfilling, stomat-surgery and other areas known to us. The topic of prevention is taking its first cautious steps [5-16]. These are, for example, the mineralization of children’s teeth, mineralization and healing of the initial forms of caries, and several experiments on volunteers (which rarely get into the open press). The discovery of hydroxyapatite-fluoride complexes, gluconate-nano-oxide pastes, hormonal and other systems that stimulate the tooth to heal itself can be considered a great success in preventive dentistry. Today, a method of similar treatment of the very first forms of caries or enamel microcracks (whitening) is recognized.
Unsolved Problems
However, this progress does not solve all “dental problems” of modern humanity. Firstly, the accumulated experience does not yet allow guaranteeing success in all cases of preventive treatment. Secondly, such dental professional points are not everywhere. Thirdly (and this is the main thing), few people go to the dentist even at the earliest stages of caries, and even more so with simple enamel whitening. Indeed, not many people are ready to spend time and money (and own nerves…) on prophylaxis in clinics, which guarantees only a distant or insignificant result at the moment (the tooth will not collapse in 10 years, the stain/microcrack will disappear).
The overwhelming majority of patients are people with pain in the teeth, large chips, abrupt changes in the bite (due to chips, etc.), fluxes and other deep lesions. As a rule, we are talking about the deepest or small, very dangerous and fast-growing carious lesions, or their consequences - large chips of enamel and dentin. The filling\prosthetic dentistry of the early 21st century does not always give an acceptable answer to these problems. For example, if the entire upper part of the tooth is damaged (with the nerve going deeper or with the remaining “single roots”), it is already impossible to talk about any fillings and pins. The tooth is removed by a dental-surgeon, despite the fact that acceptable prophylaxis and possible self-crystallization could extend its life.
Obsolete Methods and Views
As know [2-16], dentin is a natural polymer composite with a high degree of inorganic component - up to 70% hydroxyapatite and silicates. The rest is natural collagen polymer. The enamel has practically the same chemical composition, but with a higher proportion of inorganics, which is why its Mohs hardness is 6-6.5. This is higher than glass and steel (4-5 according to Mohs), but much lower than quartz (8). Which is why we have many problems with chipping and damage to teeth when accidentally biting stone (mainly quartz-granite) or bone ( with silica edges) particles in food. Previously, it was believed that, unlike enamel, dentin does not have the ability to self-repair (or has lost it during evolution). This seems strange, given that our mammalian relatives (and even more reptiles) have excellent positions here. Crocodiles change their teeth dozens of times in a lifetime. So, in mice and hamsters (although they live only 2-3 years), teeth grow like skin and bones (in humans). Cases of overgrowth of dental tissue (including in the wrong direction with the formation of thorns) are also known in cows and horses. It cannot be that the human body was so weak that it lost forever this ability, which is common in wild nature.
Most likely, this function is either in hibernation, or cannot be realized in urban conditions - due to a lack of “building material” in the dental cavity itself or in the tissues that feed the tooth. The successes of recent years in matters of enamel re-mineralization directly indicate the possibility of remineralization (albeit partial) of dentin, even with very deep lesions. But practical dentistry in the issue of treatment and elimination of the consequences of caries still adheres to the principles of 50-100 years ago. So, it is often believed that a carious cavity can be cured only by significant removal of the affected tissue, up to completely healthy tissues, followed by a filling. If such removal involves the removal of a nerve, it is removed without hesitation. If all this is difficult, the patient can also safely be sent not to remove the tooth. Like this we remove the part of the apple rotten or spoiled wormy (or apple is simply thrown away). This practice is reminiscent of the outdated practices of other restorative industries with which dentistry can be somewhat comparable.
Here are Examples from the Road, Construction and Other Industries
Earlier in build-construction, fungus in the walls was removed only by removing a very significant layer of plaster and even the wall (with subsequent cementation of the cavity). Often it turned out to be difficult, and then the affected fragment was replaced with a new block (or even the house was declared unfit). All these timeconsuming processes are largely in the past, thanks to the latest fungicidal and bactericidal primers, the method of UV\radiationexposure, and other innovative methods. Also, the restoration of products has long been using methods of impregnation of cracked or damaged fragments, rather than total “amputation” of them with replacement with new copies. In road repairs (very conservative), the old costly methods of replacing and patching road cavities (completely cutting off the old layer and applying a new one, etc.) are a thing of the past. Now in use (in developed countries) polymer-concrete and other special compounds, poured into the cavity and polymerized there.
However, there remains an effective and “popular method” of filling road pits with ordinary rubble or construction waste, followed by its self-subsidence and partial curing (pressing). The operating conditions of the teeth can also be compared to the operating conditions of tires, soles and incisors. Common is rapid corrosion after micro-damage (unless repaired by linings). Carservice has been using rust-converters for several decades). They have become powerful competitors to the traditional methods of completely cutting-off a rusted or otherwise corroded fragment in car, with the application of fiberglass or metal linings. Modern rust-converters now do not even require preliminary cleaning or degreasing of the place: the liquid turns rust, together with dirt and other deposits, into a relatively strong crystallization.
An Attempt at a Literary Review
It is difficult to conduct a qualitative review on this topic due to the lack of the necessary publications. Most often, dentists (despite serious progress in improving the quality of filling cements) and the scientists who serve them still remain in the wake of the old methods. Which are really convenient - but not for all patients (especially the poor and remote from clinics), as well as for doctors. Even the terms “self-hardening”, “self-healing”, “prophylactic” - refer to dental filling and prosthetic masses [2-6] - but not really preventive (preventing filling and prosthetics) systems. Today, in the available literature, there are lack of scientific sources on natural prophylactic formulations (homeopathic, self-crystallizing in the cavity, etc.). There are several reports of Nanobiomaterials [8], prophylaxis with antibiotics [9] or artificial compounds for self-build-up of micro-damage to the enamel [7]. Also, on the world market there are more than 10 proven toothpastes with enhanced protective and anti-carious activity. They are presented as “superinnovative” formulations from the world’s leading institutions for enamel protection (in rare cases - restoration of damaged areas of the tooth [14]).
Advertisements often contain phrases like “active calcium”, “liquid enamel”, “innovative glycerophosphate (amino-, gluconato-) calcium complex”, etc. [12-15]. However, a simple analysis of these pastes shows ordinary toothpastes compositions, only with an increased content of active components (hydroxyapatite, sodium monofluorophosphate, glycerophosphate and calcium gluconate). Like ordinary toothpastes, they (obviously - for custom attractiveness) contain components that are unnecessary and potentially harmful to the teeth - aroma, dyes, aspartame, surfactants and detergents. These commercial gels [6,12-15] do not contains natural ingredients (herbal powders, natural mineral micro-nano-particles) & nano-SiO2 or nano-Al2O3. Meanwhile, even bad dentists are not always and not everywhere enough to solve the problems of the population. In a number of cities and villages, the network of Stomatological services is either insufficient or unacceptable (not cheap, travel far, queue a month in advance, etc.).
In other cases, the dentist chooses a more convenient option for the removal of a tooth or nerve (followed by expensive imposition of bridges, pins and implants). It is high time to raise the issue of the prevention of Stomatological diseases, and even about effective methods of self-healing of carious and other lesions - by analogy with other restoration industries. In the last 20 years, we have carried out a significant range of works on the creation of acrylic polymer composites with nano-SiO2 for filling and prosthetic dentistry [2,7,16-18]. The resulting product was sold in Eastern Europe and the ex-USSR in the form of the Oxomat and Oxomat-Dipol trademarks. The Institute of Surface Chemistry took part in the development of Ukrainian toothpastes. However, on the issue of self-restoration compositions, we also do not have substantiated publications. It’s time to fix this flaw. The first results of the experiment have already been given by us in the abbreviated abstracts of the European conferences [10-11]. They are published as an article for the first time.
Simplified Problem Statement
There are many theories about tooth decay (an overview on this topic may be presented separately). However, it is possible to single out a number of general simplified provisions, from which it is relatively easy to obtain the first ways to solve problems of prevention. Tooth decay can be simply compared to the destruction of other systems that endure extreme stress. These are, for example, car tires and boot soles, pliers and secateurs; highways with busy traffic and bad climate; Polymer materials under load and lighting, etc. Common to the carious process are the stages of appearance of lesions in the integrity of products / coatings. This is, oversimplified:
1) Loss of components that ensure the integrity of dental structure. In polymers, this is leaching/degassing of the plasticizer/ stabilizer, destruction of polymer chains into shorter ones, salting out and precipitation of filler microparticles. In road surfaces, this is the loss of elasticity of the tar component of the asphalt. In teeth, this is demineralization of dental tissue and enamel.
2) The appearance of micro- and nano cracks, defects and protocavities. In tooth enamel, this is particularly manifested by discoloration (whitening).
The Idea of the Experiment
The idea of this work is the assumption of a high self-protective and even self-restorative ability of both the enamel of the teeth (which has already been proven earlier) and the dentin itself. Figure 1 schematizes the possible self-healing process when applying (or rubbing) powders and pastes with components of “building materials” for restauration. Experimental dentistry and medical chemistry today prefer to operate with nano-objects (nanohydroxyapatite, nanosilica, colloidal chalk, etc.). However, the complexity of obtaining and the high cost of nano-components force us to look for a way of simpler compositions. If we assume that the tooth itself “chooses” the necessary particles from the offered ones (and the rest will self-remove), then it is quite possible to use any poly-dispersed powders. Another obscure aspiration of the current preventive dentistry is the multicomponent nature of commercial toothpastes. They usually contain an inert filler (nanoor micromel, calcium carbonate), supplied with many additives and additives of dubious utility (saccharin, aspartame, potent surfactants, stabilizers and preservatives). For this reason, many pastes are not recommended to be left without thorough rinsing. Figure 1 shows how simple and effective the natural scheme of self-healing cavities is at any stage of development. This is of course real only if
A) High immunity (at least local);
B) The presence of “correct building materials” in the field of dental tissues;
C) Regular high hygiene in the area of the affected area;
D) Acceptable self-attitude towards a positive result;
E) Other individual factors (climate, lifestyle, regularity of procedures, individual characteristics).
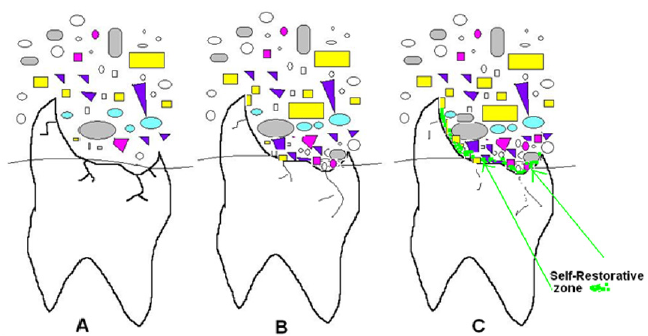
Figure 1: Scheme of the Dental “self-repair” - the most probable mechanism of self-restoration with the help of micro- and nanoparticles that accidentally or systemically fall into the tooth cavity.
In real life, as a rule, we have lack of several of their points. As a result of which the self-restoration mechanism slows down to a complete stop or goes unnoticed (for example, building up 0.5-1 microns per year). More often, the contrary situation is realized -when, instead of self-healing, there is self-wear and tear - which we observe often on the radiographs of the dentist.
The First Results of the Experiments
This can be illustrated by X-ray images of the severely damaged upper left tooth No 7 in Patient-A. At the stage of the breakaway of a large part of the enamel (Figure 2A & 2B) due to the caries under the filling (plombiring), a re-filling was carried out (Figure 2C). However, the filling turned out to be too large (and was in contact with the gum) and fell out after 2 weeks (3.2.2021). After that, the attending dentist and dentists of other clinics refused to refill it and even pinning (and sent the patient to remove the tooth). Strong, including at night Periodic, moderate Rare, weak (with general weakening) (Table 1). According to modern views, the exposed dentin in the gums is unable to withstand either loads or the action of aggressive liquid media, and must quickly collapse, with subsequent inflammation of the adjacent areas, and infection of adjacent teeth. However, the Patient accepted the scheme of selfhealing and partial restoration of tooth residues proposed by us (with powders based on herbs and nano-oxides, rinsing, etc.). By this time, the tooth represented a bare root in the gum, cleaned “for filling”, with a 2 * 2 mm particle of enamel protruding above the gum.
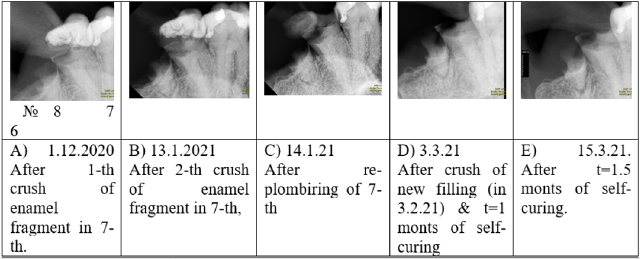
Figure 2: X-ray (Rentgen-Putuylampe) photo of investigated zone of 6,7 & 8 teeth.
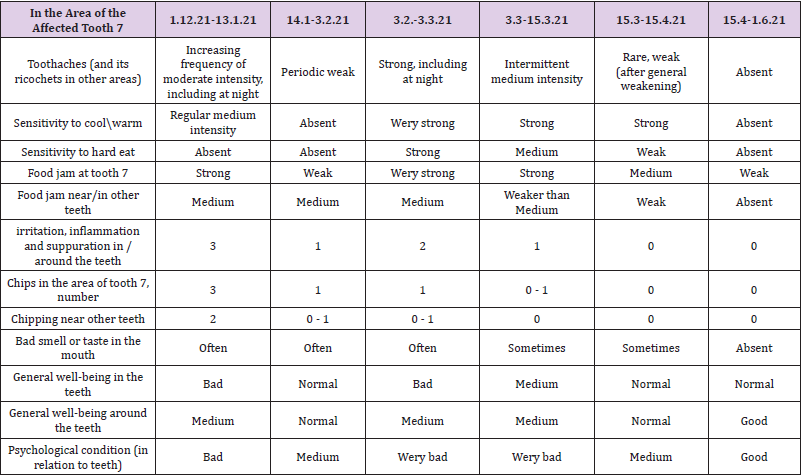
Table 1:Patient-A’s well-being during the observation period (1.12.2020 - 1.6.2021). Absent - no sensations or they are normal.
A month later, on 3.3.2021, the Patient-A returned to the clinic and performed an X-ray in order to find out the degree of root damage by caries (since the tooth began to feel more strongly chilling and hard food, and sometimes pain). In case of deepening caries, the patient was ready for immediate removal. However, to the surprise of the doctors observing the tooth, no negative changes (tooth chipping, carious zones, tooth holes) were observed (Figure 2D). On the contrary, self-closure of all adjacent interdental areas is seen from the X-ray photograph (compare Figure 2D & Figure 2A, 2B, 2C). In addition to that, it is clearly visible above the 8th tooth (also a destructed root in the gum) (Table 2). This is illustrated by the typical successful outcome of self-restoration processes with the proposed compositions in Patient-B (a 7-year-old child, Figure 3). Lateral teeth 1,3 and 4 - were processed; tooth 2 - was not processed and began to completely collapse. Now we are carrying out a special treatment of it, which stopped further destruction. Another typical story is related to complaints of hypersensitivity, brittle teeth and regular stuck of any food in the teeth and between them (a typical situation for the majority of the world’s population).

Table 2:The number of recorded effects, according to estimates in the experimental groups.
Dentists in such cases recommend expensive stepwise treatment (desensitization, prosthetics, filling, etc.). After applying our course, the patient (hereinafter Patient 2), already the next month, noted the termination of the jam of any (including fiberneedle fragments, orange, cake and other particles) food. The next month, the increased sensitivity of the enamel stopped. According to Patient-B, he feels that the enamel is “covered with a fine hard dusting”. Six months later, he noted the absence of any chips and spalls during chewing, as well as the ability to gnaw random aggressive inclusions (parts of pebbles, bones, etc.) with his teeth without consequences. As an example, we can also cite the strengthening of the lower molars in a schoolchild (Patient 3) after prophylaxis with our powders (in combination with toothpastes and rinses with sage and mint infusions). They were affected by primary or secondary (after filling) caries, and at the beginning of 2021 they were sensitive to hot and cold. By the summer of 2021, there are no pathological sensations in these teeth, they work normally under any load; their appearance also changed (dark carious spots disappeared).
Discussion on the Results of the Experiment
Method Limitations
With all the positives, one must understand the limits of the possibilities of self-healing. The use of the declared methods significantly expands the boundaries but does not cancel them. Table 3 shows the main limitation - the impossibility of (fast) growth of dental tissue in volume - especially lateral chips and deep lesions. This function will continue to be at the mercy of official dentistry and artificial polymer-composite materials. Indeed, selfrepair technologies with “friendly” micro-nanoparticles operate with micron-sized coatings. In the best case, blurring and selfovergrowing of round (surrounded by dental tissue) cavities of any depth is possible (which is noticeable in the molars in Figures 3 & 4). Build-up of side chips, leading and cutting edges, etc. - much more effective in the dentist’s chair. The possibilities of self-help for very deep lesions (flux, periostitis, etc.) and anaerobic inflammation under the filling have not been studied either. In these cases, external influence may be useless or too slow.

Table 3:Some features of the “self-repair” method (estimation).
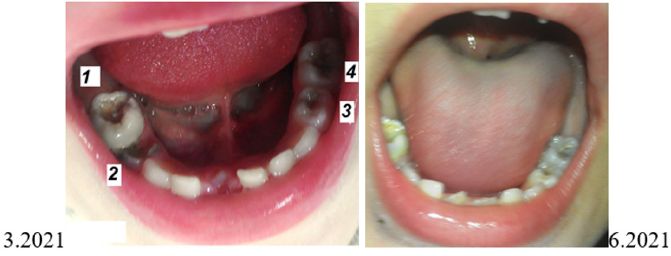
Figure 3: Visual info on self-repair. Molars and posterior teeth of Patient-B. 1,3 and 4 - were processed; 2 - not processed and destroyed.

Figure 4: Left lower lateral in a 10-year-old child (Patient-C) - an example of strengthening (cessation of secondary caries and sensitivity to hot / cold) after the declared prophylactic treatment.
As you can see, all the limitations are similar to those we have with skin lesions. We treat small cuts and even suppurations ourselves (iodine, brilliant green, ointments, medical glue, adhesive plaster, etc.) - and this is up to 80% of all injuries. But deep and non-healing wounds, trophic and gangrenous lesions are better not to trust self-medication. We are talking about how to “pull up” dental self-prophylaxis to the usual standards of self-profilaxis of skin injuries. In the meantime, people with the slightest dental issues - either immediately run to the dentists (who often immediately operate and violate the delicate balance), or do not pay any attention until major problems appear. Now, almost every toothpaste marketed is claimed to be “anti-caries” or “preventative.” This is partly the case in the segment of expensive and premium goods. But we must take into account the rate of the majority of the population on the cheapest segment. And these are usually aromasweetened (which is already harmful to the teeth) microdispersed CaCO3 and SiO2 (which is ineffective) or even gypsum-chalk (which is harmful) mixtures.
Comparison with Dominant Methods and Attitudes
Now, almost every toothpaste marketed is claimed to be “anticaries” or “preventative.” This is partly - the case in the segment of expensive and premium goods. But we know - the majority of customers buy the cheapest segment of toothpastes. And these are usually aroma-sweetened (which is already harmful to the teeth) microdispersed CaCO3 and SiO2 (which is ineffective) or even gypsum\chalk (which is harmful) mixtures. Also, you should take into account the lack of the correct culture of using toothpastes. The overwhelming majority of people (including the dentists themselves!) Retain their acquired habits from childhood. For example, treat your teeth as an alien hostile element of your body, ready at any moment (usually at the most inappropriate) to betray and strike (break, rot, get sick). The dentist is seen here as a miraculous savior - even when it comes to the complete removal of a nerve or even a tooth. At the same time, few people even think to assume that teeth have no less regenerative power than, for example, skin, bones, eyes, hair or blood vessels.
There are also known regions where people do not get caries at all - albeit with an ultra-low culture of dental care. The foregoing suggests that the teeth can easily repair most microdamages on their own - if they are given “building material” and freed from mechanical (chewing too hard/elastic, hot/super cold) and sanitary problems (domination & remnants of carious food, acidic food/ drink, etc.). It is evident that in many cases even filling can play the opposite role - just as a hermetically applied plaster or medical glue stops the healing processes on the skin and activates putrefactive inflammation. Dental tissue is an open system and sealing it with a filling or crown inevitably leads to known complications under the prosthetic onlays (and this is a recognized problem that has caused the emergence of dental creams such as Corega). Meanwhile, by activating the healing potential of the tooth, it is theoretically possible to achieve partial (sufficient for -\+ normal life of the tooth) self-healing.
In areas with insufficiently developed dentistry, we often can meet people with problem or dilapidated teeth, which, however, continued to function. When oral examining of village-people, in place of the teeth, it possible to find: gum growths, thickenings or even gray-brown growths directly on the affected (or formerly affected) areas of the teeth or their remnants (“stumps”). They serves as a forced “natural seal” from scrap materials (dust, plant fibers, microparticles of sand and limestone, etc.). The lifespan of such self-substitutes is obviously very different, but it can reach many years. There have been cases when the replacement of such “ugly” (but working and not disturbing) formations with “beautiful fillings” or whitening from the dentist led to a rapid or gradual collapse of both the tooth itself and the adjacent teeth and tissues. Of course, such self-healing is possible in places with an acceptable composition of “good dust” in air, dental powders & foods, and with a certain immune response in the patient-s organism. Most likely, every dentist (and even an ordinary person) in life has met such cases among people who have come into contact with him. It remains only to put these facts on the basis of scientific research and expand the base of mineralizing prophylactic pastes and preparations for deep lesions and tooth decay.
Approximate formulations of prophylactic and restorative powders from commonly available components.
1) Coniferous Powder: The needles and cones (if necessary, washed and dried) are ground with a coffee grinder. The fine fraction is sieved through a sieve and used. A suitable amount (1:1 or 1:2) of nano-dispersed SiO2 (pyrogenic silica) is added to the mixture, if possible, nano-Al2O3, nano- or micro CaCO3 (or commercial tooth powder). Due to coniferous resins, the effect of fixing nano-microparticles in the pores and cavities of the tooth is enhanced. In this case, coniferous components enhance the disinfecting effect, and nano oxides - the sorbing effect. If desired, you can add a small dose of water-hardening micro-silicates (cement, white clay) or other components (gypsum, quartz).
2) Tea Powder: After use, the brewed tea is dried and crushed in a coffee grinder. Next, nano- and micro-inorganic components are added (as in claim 1).
3) Mint Powder: The mint is dried and ground in a coffee grinder. Next, nano- and micro-inorganic components are added (as in claim 1).
4) Sage Powder: The shavings purchased at the pharmacy are crushed. Next, nano- and micro-inorganic components are added (as in claim 1).
5) Hop Powder: The hop cones are collected, washed and dried. Further - as in paragraph 1.
These powders can be freely mixed, add a fine fraction of other medicinal herbs (cinnamon, oak bark, coriander, rosemary, mint), at the request of the user. When cleaning with such powders, it is not necessary to rinse thoroughly right away. On the contrary, their beneficial effect will last if left on the teeth for a comfortable time. For example, rub-in powders can be left overnight and rinsed out in the morning. These methods are very convenient in the field, as well as for children when rinsing is difficult (for example, outside the bath or if the child almost fell asleep forgetting to brush his teeth). The combination of these powders with toothpastes & remineralisators (which have inaccessible and clinically proven components such as fluorides and hydroxyapatite) apriority can enhance the self-restorative effect.
Conclusions
1) Biomedicine has a large body of evidence on the regenerative capabilities of bone and dental tissues. This resonates widely in the household sector - especially in regions with undeveloped or expensive dentistry. However, as applied to teeth, this topic has not yet found development, as evidenced by the absence or lack of regular data in scientific periodicals.
2) The regular scientific experiments on self-regeneration of dental tissues at any degree of damage, were done. It has been shown that the use of powders and pastes based on micro(nano)particles of plant and mineral origin makes it possible to obtain acceptable or unexpectedly good results in eliminating pathologies and problems of teeth and arounddental tissues.
3) Based on the results of the first studies, approximate methods of self-restoration were proposed without consulting specialists. Several recipes for making self-restoring tooth powders based on commonly available components are presented.
Acknowledgments
1) Special thanks to the doctors of dental clinics:
a) Andrey Kladiyov (head of the department of dentistry in Center №3 for Primary Health Care of the Svyatoshinsky District of Kiev, Rykov str.,2) - a high master of filling and pinning with photopolymers, who provided an X-ray visiograph for regular examinations. Despite the skepticism and conservatism inherent in doctors, he patiently listened to my reasoning and even gave some advice.
b) Y. Palamarchuk (doctor stomatologist with 50 years of experience in the Kiev’s Dental Clinic, Antonova str.8), - a super-dentist who knows how to restore completely hopeless teeth by filling, easily extending their service life for another 10-40 years. His skill, advice and remarks inspired me to do this business. Also, thanks to his colleague, orthopedist Y. Didenko, who also gave some advice on this topic. 2) Experimental volunteers who agreed to these experiments without much hope of success and are still surprised by the results.
3) Ph.D. N Shklovska, Lead. Engin. Т. Solovyova & Lead. Eng. A. Petranovskaya - The creators of Soviet and Ukrainian photopolymer prosthetic-filling composites (TM Oxomat- Dipol), who were among the first world developers of modern light-hardening compositions and toothpastes based on nano- SiO2. I had the privilege of completing a thesis in this innovative team in 1991-2004. Also, thanks to the first Director of the Institute Doct. Sci., Prof. Chuiko A. and Vice-director Prof. V. Pokrovsky, who supported the defense of this dissertation in 2001-2004 - a period of temporary cessation of state funding for these works after the destruction of the Soviet Union. 4) The Editorial Board of Biomedical Journal of Scientific & Technical Research, which agreed to print this article without major changes and at a price that is acceptable to us.
References
- V Veresaev (1961) Doctor's notes (Zapiski vracha) . Moscow, (Edn.). PRAVDA.
- DL Starokadomsky (2004) Influence of highly dispersed pyrogenic silicas on the processes of photopolymerization of oligoetheracrylates and properties of the obtained stomatologic composites] (Printed In Ukrainian - Vplyv vysokodyspersnykh pirohennykh kremnezemiv na protsesy fotopolimeryzatsiyi olihoefirakrylativ ta vlastyvosti oderzhanykh kompozytiv). Thesis of Dissert. for Dr. Chem. Sci. (Kyiv: AA Chuyko Institute for Surface Chemistry, National Academy of Sciences, pp. 200).
- T Tauboeck, H Oberlin, W Buchalla, M Roos, T Attin (2011) Comparing the effectiveness of self-curing and light curing in polymerization of dual-cured core buildup materials. J Am Dent Assoc 142(8): 950-956.
- Ilie N, Simon A (2011) Effect of curing mode on the micro-mechanical properties of dual-cured self-adhesive resin cements. Clin Oral Investig 16(2): 505-512.
- Zhang Y, Wu N, Bai X, Xu C, Liu Y, et al. (2013) Hydroxyapatite induces spontaneous polymerization of model self-etch dental adhesives. Mater Sci Eng C Mater Biol Appl 33(7): 3670-3676.
- (2021) Enamel plus temp self-curing liquid.
- Starokadomskii D, Solov'eva T (2003) Effect of Small Additions of Stabilizer and Pigments on the Degree of Bulk Curing of a Filled Photopolymer. Russian Journal of Applied Chemistry 76: 616-618.
- M Hannig, C Hannig (2013) Nanobiomaterials in Preventive Dentistry; Nanobiomaterials in Clinical Dentistry.
- D Tong, B Rothwell (2000) Antibiotic prophylaxis in dentistry: a review and practice recommendations. J Am Den Assoc 131(3): 366-374.
- Starokadomsky D, Reshetnyk M (2021) Possibilities of pyrogenic nanosilica "Asil" A300 as the main component of formulations for self-restoration and delay in the development of deep carious lesions. European scientific discussions. Abstracts of the 5th International scientific and practical conference. Potere della ragione Editore. Rome, Italy, p. 21-27.
- Starokadomsky D, reshetnyk M (2021) Possibilities of pyrogenic nanosilica "Asil" A300 as the main component of formulations for self-restoration and delay in the development of deep carious lesions. The V International Science Conference. Development and implementation of technologies in production. Leeuwarden, Netherlands, p. 86.
- Dental Gel Plus, Truly Whitening, Wintergreen.
- Paro Swiss amin fluor gel. For intensive profilactic of caries. Paro Inc. Home of Swiss Manufactured Products.
- Apa Care. Remineralisated dental paste.
- O.C.S. Medical Mineralis. Remineralizing gel containing bioavailable sources of calcium, phosphate and magnesium.
- D Starokadomskii (2008) Effect of nanodispersed silica (Aerosil) on the thermal and chemical resistance of photocurable polyacrylate compounds. Russian Journal of Applied Chemistry 81 (12): 2155-2161.
- Starokadomskii DL, Solov’eva TN (2002) Effect of silicon oxide fillers on photochemical curing of compounds based on acrylic monomers and oligomers Russian Journal of Applied Chemistry 75: 138-141.
- DL Starokadomsky (2008) Some features of swelling of photopolymer composites with different contents of highly dispersed silica. Plasticheskie Massy N2, p. 33-36.
