 Research Article
Research ArticleABSTRACT
The main objective was to determine the prevalence of the fungal skin diseases and explore the related factors including demographical, personal hygiene aspect and socio-economic status of the patients, the study was performed at the Dermatology Departments of three tertiary care hospitals. Collection of skin samples and personal interviews of patients were followed by laboratory confirmation of the diseases and their pathogens were completed by direct microscopy and culture. Among 800 patients, 310 patients had fungal infection with highest prevalence [38.75%] where ringworm [81.61%] and Oral candidiasis [2.9%] were highest and lowest. Onchomycosis [27.41%] had highest prevalence among ringworm patients. In case of factors, summer season [59.68%], married [71.93%], secondary education [36.45%], 12000-20000tk monthly [38.06%] and upper-middle class status [38.06%], Muslims [86.13%], businessmen [39.73%], urban areas [69.35%], tap water [69.35%], recurrent infections [62.9%] and overcrowding of family [66.13%] had higher prevalence of fungal infections of skin. This research would add to the scientific literature and health policies as unlike other studies it has specifically evaluated the prevalence of fungal skin diseases of an urban city with associated factors in Bangladesh.
Keywords: Fungal skin diseases; Outpatients; Tertiary care hospitals; Bangladesh; Urban city
Introduction
Globally, fungal skin diseases are very common in human. As
a densely populated developing country and having poor hygiene,
sanitation practice, Bangladesh is no different to fungal skin
infections. The skin protects us from microbes and the elements of
skin help in regulating body temperature and permit the sensations
of touch, heat, and cold. As it interfaces with the environment, skin
plays an important immunity role in protecting the body against
pathogens. It is subject to a wide range of medical conditions and
infections ranging from simple manifestations to complicated ones
like skin cancer. Symptoms and severity of skin disorders vary
greatly. They can be temporary or permanent and may be painless or
painful. Some have situational causes, while others may be genetic.
Some skin conditions are minor, and others can be life-threatening.
However, fungal, bacterial, parasitic and viral infections are very
common in the healthy people. Several types of parasitic, bacterial
and fungal infections are found which causes negligible mortality
but most of the diseases have chronic course and sufferings [1].
The skin is the body’s initial defense against parasites, fungi,
bacteria, viruses and other microbes. But skin and venereal diseases
cause a large part of illness. About 50% of people in Bangladesh
suffer from skin disorders in their lifetime. Incidence of infection
on skin is very frequent due to some environmental, natural, occupational and individual habitat variations. It increases when
people are herded together and facilities for washing the body
and clothing are reduced. Recurrence, excessive use of chemicals
and cosmetics, environmental pollution, delayed marriage etc is
the major leading factors for the initiation and transmission of the
diseases.
About 80% of population in Bangladesh live in the rural areas,
where poverty, literacy, ignorance, high family members, disease
and disasters are the constant companion of them. Increasing
population, socio economic conditions have become poor and due
to this population explosion, all the reversible socio-demographic
conditions go in favor of disease occurrence, recurrence,
and complications. In addition, overcrowding, urbanization,
industrialization, migration, excessive use of chemicals and
cosmetics, environmental pollution, greenhouse effect, education,
delayed marriage and use of multiple partners are also the major
leading factors for inflation and transmission of diseases.
Skin and venereal diseases are one of the major public health
problems in developing countries. Though it occurs in all class of
society but people living in insanitary and poor housings conditions
suffer more from the disease, poverty-stricken people with poor
hygienic habits and unclean clothing are the usual victims of these
diseases. Symptoms of infection depends on the type of organisms
that has caused the infection and both symptom and appearance
also depend on the part of the body infected. In many studies it has
been shown that 30-40% of our population is suffering from skin
diseases. Of which about 80% are scabies and pyogenic infections.
Children are the worst sufferers from these diseases (Khanum
and Alam 2010). The relation between the skin and venereal
diseases of the diabetic patients of different age group and sociodemographic
characteristics is very complicated. The sociodemographic
aspects are very important to know because in
different societies and social groups explain the causes of illness,
the type of treatment they believe and to whom they turn if they go
get ill (Khanum et al. 2007).
In human anatomy, the largest outer organ, covering throughout
the whole body is skin. Skin performs a very significant role in
immunization by defending against outer microbes and pathogens.
Moreover, the elements of skin help the body to regulate the
temperature throughout the body and create the feelings of heat,
cold and touch. However, this important organ of the body has been
exposed to a variety of infections and medical sufferings varying
from simple acne to very intricating skin cancer types. Worldwide,
among human diseases, the most common is skin disease. It can
affect individuals anytime during their lifetime [1], can strike at
any age, can spread over all societies and cultures. In time skin
disease can lead to systematic disorders. Its damaging effects lead
to physical disability even death [2].
In 2010, the global burden of disease [GBD] published that
skin diseases ranked fourth as the prominent reason for non-fatal
disease burden affecting both high- and low-income countries [3].
In 2013, GBD published that skin diseases are responsible for 39
million years lived with disability [YLDs] and in case of disabilityadjusted
life years [DALYs] sit has attributed 1.79% to the global
burden of diseases [4].
Fungal Disease: Ringworm (Dermatophytosis)
Ringworm, also known as dermatophytosis or Tinea, is a
fungal infection of the skin. The name “ringworm” is a misnomer,
since the infection is caused by a fungus, not a worm. Ringworm
infection can affect both humans and animals. The infection initially
presents with red patches on affected areas of the skin and later
spreads to other parts of the body. The infection may affect the skin
of the scalp, feet, groin, beard, or other areas. Ringworm can go by
different names depending on the part of the body affected.
1. Tinea capitis [Ringworm of the scalp] is a fungal infection
affecting on scalp.
2. Tinea corporis [Ringworm of the body] is a fungal infection
that affects the skin of body.
3. Tinea cruris [Jock itch] is a fungal infection that affects the
warm and moist area such as buttocks, groin, inner thighs etc.
4. Tinea pedis [Athlete’s foot] is a fungal infection that affects
the skin of feet.
5. Tineaunguium [Onychomycosis] is a fungal infection that
affects either the fingernails or toenails.
6. Tinea facie is a fungal infection that affects the face.
7. Tinea barbae is a fungal infection that affects the beard area
of men.
8. Tinea mannum is a fungal infection that affects the area of
hands.
9. Tinea versicoloris a fungal infection that affects the whole
body as the form of discolored patches of skin.
Dermatophytosis tends to get worse during summer, with
symptoms alleviating during the winter. The disease can be
transmitted between animals and humans [zoonotic disease].
Three different types of fungi can cause this infection. They
are called Trichophyton, Microsporum and Epidermophyton. It’s
possible that these fungi may live for an extended period as spores
in soil. Humans and animals can contract ringworm after direct
contact with this soil. The infection can also spread through contact
with infected animals or humans. The infection is commonly spread
among children and by sharing items that may not be clean. Fungi
thrive in moist, warm areas, such as locker rooms, tanning beds, swimming pools and in skin folds. It can be spread by sharing sport
goods, towels, and clothing.
Symptoms and severity of skin disorders vary greatly. The
consequence of this problem is serious for the patient as well as
for the society. Among skin diseases, fungal, bacterial, parasitic
and viral infections are very common. The distributional pattern of
skin diseases varies widely from country to country, even within
the country itself [1]. Although they are attributable to a very
insignificant mortality rate but most of the skin diseases comes
with a possibility of prolonged sufferings thus raising public health
concerns in developing countries.
Bangladesh is a densely populated country with 164.69 million
population and 24% of people live under the poverty line [5] and
the majority of the population suffer from different infections and
contagious diseases. Study conducted by Khanum and Alam, it has
been shown that 30-40% of our population is suffering from skin
diseases [6]. Approximately, 40% of people live in urban cities and
the highest 10.3 million people live in Dhaka city [7]. Several papers
have studied common skin and venereal diseases in Bangladesh
[8-14] but our paper is specifically concerned about fungal skin
diseases and their associated factors in three tertiary care hospitals
of an urban city, Dhaka, Bangladesh.
According to the 2010 GBD, fungal skin infections were among
the top 10 most dominant diseases globally [3]. According to the
2013 GBD, 0.15% of DALYs of the global burden of skin diseases
are contributed by fungal skin diseases [4]. In rural areas of
Bangladesh fungal skin infections are very common [15]. A study
on the common skin diseases revealed that out of 440 patients 13%
had fungal infections [11]. Other studies of Bangladesh showed
prevalence ranging from 15.5%- 26.7% [12-14]. India, neighboring
country to Bangladesh also reported that Fungal diseases were
the highest group of all skin diseases with 18.74% prevalence [16]
and second highest with 17.19% prevalence [17]. In Pakistan, a
study conducted in 2017 showed 34.80% prevalence of fungal
skin infections out of 95983 patients in a tertiary care hospital of
Karachi [18]. A community-based survey studying the skin diseases
of South Asian Americans found that fungal had 11% prevalence
after Acne and Eczema [19].
Numerous factors can influence the prevalence of skin
infections mentioning geographical and cultural factors [20-21],
educational status, nutritional status, socio-economic status, as well
as seasons, overcrowding, unhygienic habits, and environments are
significant factors of defining the distribution of skin diseases in
developing countries [1,22-24]. The socio-demographic aspects are
very significant to know because in different societies and social
clusters rationalize the reasons of illness, what types of treatments
and whom they believe in case of their treatments [5].
Materials and Methods
This research study was performed at the Dermatology Department of the Bangladesh Institute of Research and Rehabilitation in Diabetes, Endocrine and Metabolic Disorders [BIRDEM], Dhaka Medical College and Hospital [DMCH] and Uttara Adhunik Medical College and Hospital [UAMCH]. The study was undertaken from 25th March 2018 to 10th February 2019. A total of 800 outdoor patients were randomly selected of all genders, ages, sexes, with different occupations irrespective of their skin problems during the data collection period of BIRDEM, DMCH, and UAMCH. The present study was conducted in two steps, firstly collecting samples and data through personal interviews and secondly laboratory confirmation of the diseases and their pathogens. A literature review was carried out about the factors relating to skin diseases before a structured questionnaire was prepared for interviewing the patients about their demographics and socio-economical aspects.
Statistical Analysis
Analysis of the data has been achieved by using the statistical software SPSS [version-20.0] and the results were presented in percentages. We have matched our results with comparable studies of other cities of the country and nearby countries through similar hospital attendance-based studies.
Ethical Approval
We informed each and every patient about our study aims, methods as well as we assured them about their privacy and confidentiality at any stage of the study [at the time of data, sample collection and laboratory diagnosis] before including them into our study. We also made it flexible to the patients to enter the study and also to withdraw their consent.
Results
In the present observation cross-sectional study has been
outlined to determine the prevalence of the fungal skin diseases
of tertiary care hospitals in an urban city. The present study also
provides a descriptive profile of factors related to the fungal skin
diseases including demographical, personal hygiene aspect and
socio-economic status of the outpatients attending the Dermatology
Department of major three tertiary care hospitals in Dhaka city,
Bangladesh.
There were a combination of skin infections including fungal,
viral, bacterial, parasitic, sexually transmitted diseases [STD]
but maximum patients had fungal skin infections. Among the
800 patients, 310 patients were infected with fungal infections
[38.75%]. It was observed, of those 310 patients 183 [59%] were
male patients and 127 [41%] were female patients. Out of 310 fungal infected patients, most of the patients, were infected by
ringworm [81.61%] and the lowest prevalence was found in case
of Oral thrush [2.9%] (Table 1). Besides, ringworm patients were
infected by Pityriasis versicolor, Seborrhoeic dermatitis. Among
253 patients of ringworm patients the highest prevalence was
found in case of Onchomycosis [21.94%] and the lowest prevalence
was found in case of Tinea capitis [0.97%] (Figure 1).

Table 1: Prevalence of fungal skin infections of skin among the patients.
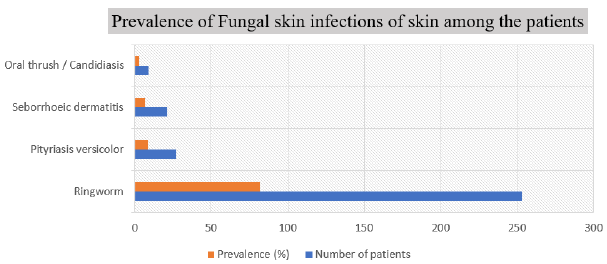
Figure 1: Prevalence of ringworm causing agents among the patients.
Among the 183 male patients highest 66.67% were infected by Oral thrush/ Candidiasis and lowest 42.86% were infected by Seborrhoeic dermatitis whereas, among the 127 female patients highest 57.14% were infected by Seborrhoeic dermatitis and 33.33% were infected by Oral thrush/ Candidiasis] (Table 2). Moreover, in ringworm causing agents highest 67.65% male were infected by Tinea pedis and lowest 20% males were infected by Tinea facie while in female group highest 80% were infected by Tinea facie and lowest 32.35% were infected by Tinea pedis (Table 3).

Table 2: Prevalence of fungal skin diseases according to the gender of patients.
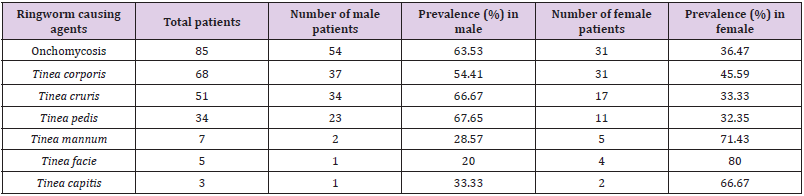
Table 3: Prevalence of ringworm causing agents according to gender of patients.
It was also observed that out of total 310 fungal infected patients, the highest burden of fungal infections was present among the patients of age group of 31-45 [32.26%] and the lowest burden of infections was belonged to the patients of age group of 0-15 [6.13%] (Table 4). This was also similar for the prevalence of the specific ringworm causing agents. Age group of 31-45 years had highest prevalence [32.81%] and 0-15 years group had lowest prevalence [4.74%] (Table 5). Finally, we observed the factors from the personal interviews of the 310 patients mentioning marital status, socio-economic status, educational status, monthly income, occupation, seasons, religions, sources of water, residence location, regular bath, regular types of clothes, personal items sharing, history of recurrent infections, times of recurrent infections, overcrowding of family (Table 6).
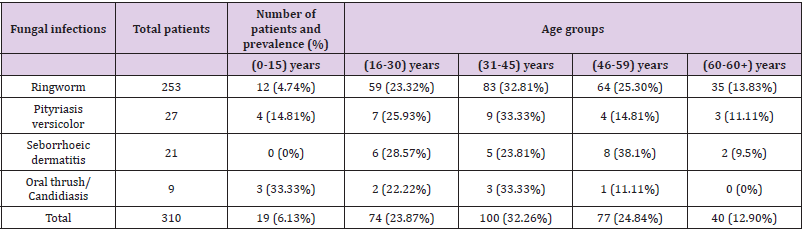
Table 4: Prevalence of fungal infections in different age groups.
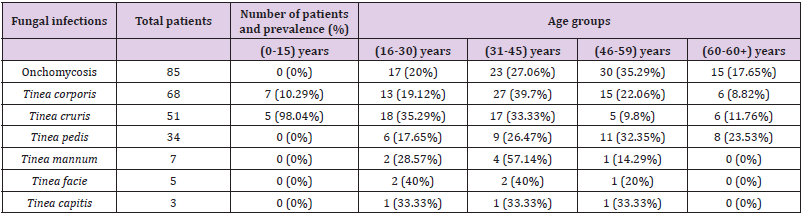
Table 5: Prevalence of ringworm causing agents in different age groups.
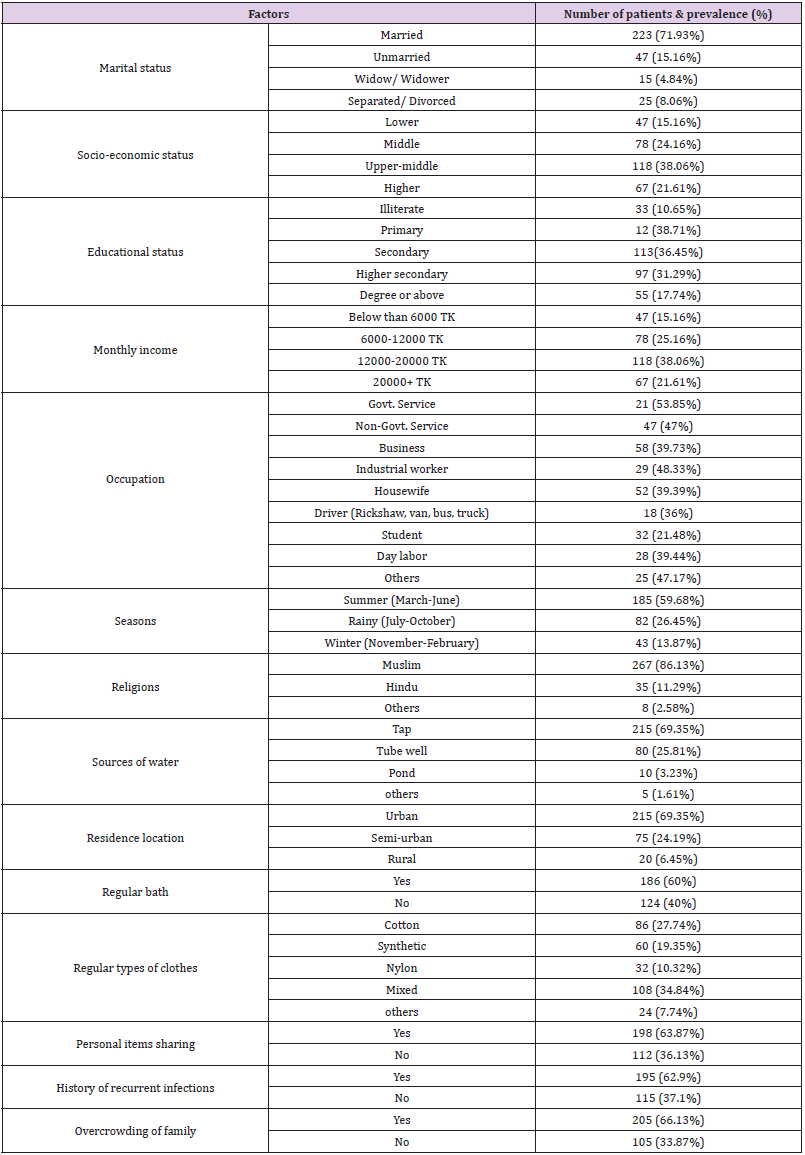
Table 6: Prevalence of fungal infections according to considered factors.
Discussion
In the present investigation, out of total 800 patients, 310
patients had fungal infections with the highest prevalence [38.75%]
followed by other fungal skin problems. Out of fungal infections
ringworm had highest prevalence [81.61%] followed by Pityriasis
versicolor, Seborrhoeic dermatitis and Oral thrush/ Candidiasis.
Among the ringworm, onchomycosis [27.42%], Tinea corporis
[21.94%], Tinea cruris [16.45%] had the highest prevalence. It was
also observed were male patients had high prevalence [59%] than
female patients [41%]. In case of age group patients contained
among the age group of 31-45 had the highest [32.26%] and the
lowest prevalence of patients belonged to the age group of 0-15
[6.13%]. Outcomes of this study are similar to results of some
studies while contradicts to some.
In 1993, a study performed by Hossain [25] found that fungal
infection [20.19%], and seborrhoeic dermatitis [8.80%] were most
common among the skin diseases [25]. In 1995, Bahmadan et al.
[22] reported that in Abha city from Saudi Arabia among the fungal
disease developing pathogens, Tinea capitis [9.6%] and Tinea
pedis [1.9%] were most common [22] but we found Tinea corporis
[21.94%], Tinea cruris [16.45%] had the highest prevalence. In
2011, a study conducted by Rahman et al. found Tinea corporis
[22.63%] was the most frequent infection as well as males were
mostly infected with fungal infections which is similar to the results
of this present study [15].
In 2007, study by Khanam et al. informed that among the fungal
infected patient’s majority [42.7%] were infected by ringworm,
45.36% by Pityrious versicolor and lowest [12%] were infected by
Candidiasis. Khanum also reported that the prevalence of fungal
infection was in highest in 40-49 age group [25.33%] and less in
20-29 age group [14.66%] and prevalence in male was highest
[61.33%] than female [38.66%] [8]. In 2012, one study from a
Dhamrai area near Dhaka performed by Nafiza et al. had reported
that among the patients with cutaneous skin diseases, fungal
infections were the commonest and highest [22.9%] and males
had high prevalence [63.4%] than females [36.6%] [12]. In 2017,
Haque et al. revealed among the 504 patients who were surveyed
from Rajshahi, an unbar city of Bangladesh with different types of
skin disease, male had highest prevalence of fungal infections [26].
In this present study we had explored not only the
demographical and socio-economic aspects but also seasonal
aspect and the hygiene habits of the patients to better understand
the factors related to the fungal skin diseases. It has been witnessed
in. this study, that among the fungal infected patients who were
married [71.93%], had secondary education [36.45%], earned
12000-20000tk monthly [38.06%] and had upper-middle class
status [38.06%] had higher prevalence. Moreover, patients who
were Muslims [86.13%], had businesses [39.73%], lived in urban
areas [69.35%], used tap water as the source of water [69.35%]
also had higher prevalence of fungal infections of skin. In case of
personal hygiene of the patients, who wears cotton clothes regularly
[27.74%], baths regularly [60%], shares personal items [63.87%],
had recurrent infections [62.9%] and had overcrowding of family
[66.13%] had higher prevalence. Additionally, in summer season
fungal infections had higher prevalence [59.68%]. This study had
found high prevalence in Muslims as the study was conducted in an
Islamic country.
There are several studies conducted in Bangladesh had found
different results than ours. According to them, the prevalence was
higher is rural areas [15], among students [10], patients from low
socio-economic status [9], among illiterate patients [9,10], in rainy
season [8]. According to Khanum et al. 52.16% of the patients
with low socio-economic status showed a high reoccurrence of
skin disease which contradicts our study result [8]. From these
observations it can be said that skin infections in patients is very
frequent in urban regions even if the urban cities of the country
have improved standard of living, hygiene and sanitation, better
quality healthcare facilities, education, and nutritious food to lessen
the fungal skin diseases rather than the rural part of country. So, the
present study has tried to give an approximate fungal skin disease
prevalence scenario with related factors of the whole country.
Conclusion
Present cross-sectional study has provided some unique results and findings which would add to the scientific literature and health policies as it is first of its kind. No other research work has evaluated the prevalence of fungal skin diseases of an urban city with associated factors in Bangladesh. Moreover, this work can also be scaled up to other pathogens of skin diseases. However, there is no vaccine against skin diseases it is very difficult to control its transmission so to control this disease is to improve socioeconomic condition, change the personal hygiene behaviour and taking appropriate preventive measures.
Conflict of Interest
No conflict of interest with any institution/organization.
References
- Rook A, Savin JA, Wilkinson DS (1987) The prevalence, incidence and ecology of diseases of skin. In: Rook A, Wilkinson DS, Ebling FJ, Champion RH, Burton JL, editors. Textbook of Dermatology. Mumbai: Oxford University Press: Mumbai: p. 39-53.
- Basra MKA, Shahrukh M (2009) Burden of skin diseases. Expert Review of Pharmacoeconomics & Outcomes Research 9(3): 71-283.
- Hay RJ, Johns NE, Williams HC, Bolliger IW, Dellavale RP, et al. (2014) The Global Burden of Skin Disease in 2010: An Analysis of the Prevalence and Impact of Skin Conditions. Journal of investigative dermatology 134(6): 1527-1534.
- Karimkhani C, Dellavalle RP, Coffeng Le, Flohr, Carsten, et al. (2017) Global Skin Disease Morbidity and Mortality an Update from the Global Burden of Disease Study 2013. JAMA Dermatol 153(5): 406-412.
- (2020) ADB: Asian Development Bank. ADB and Bangladesh.
- Khanum H, Alam S (2010) Occurrence of Scabies among the Out-patient Children of Dhaka Medical College, Dhaka. Bangladesh J Zool 38(1): 7-11.
- (2020) WORLOMETER. Bangladesh population.
- Khanum H, Khanum P, Farhana R (2007) Common skin diseases in relation to socio-demographic status among the outpatients in the department of skin and venereal disease of DMCH, Dhaka. Bangladesh J Zool 35(2): 391-396.
- Uddin MR, Sarwar KB, Akhter F, Baker A (2011) Pattern of Dermatological Cases Attending Skin-VD Outpatient Department in a Medical College Hospital of Bangladesh. J Enam Med Col 1(2): 67-70.
- Yousuf AKM, Joarder Y, Aktar A, Hoq MN, Rahman M, et al. (2013) Pattern of skin diseases in patients attended OPD of Dermatology and Venerology in a tertiary care teaching Hospital in Bangladesh. Bangladesh J Physiol Pharmacol 29(1&2): 8-11.
- Ahmed AM, Haque M, Sadir AM (2003) Pattern of skin diseases in the patient of department of Comilla Medical Collage Hospital. J Comilla Med Coll Teach Assoc 5(1): 6-12.
- Nafiza A, Islam MZ, Farjana S (2012) Pattern of Skin Diseases: Experience from a Rural Community of Bangladesh. Bangladesh Medical Journal 41(1): 50-52.
- Sarkar SK, Islam AKMS, Sen Kg, Ahmed ARS (2010) Pattern of Skin Diseases in Patients Attending OPD of Dermatology Department at Faridpur Medical College Hospital, Bangladesh. Faridpur Med Coll J 5(1): 14-16.
- Alahi MN, Hossain MA, Mohammad AS (2018) Pattern of Skin Diseases in Patients Attending OPD of Dermatology and Venereology in a Tertiary Care Hospital in Bangladesh. Journal of National Institute of Neurosciences Bangladesh 4(2): 116-122.
- Rahman HM, Hadiuzzaman M, Bhuiyan MD, Islam N, Ansari NP, et al. (2011) Prevalence of superficial fungal infections in the rural areas of Bangladesh. Iran J Dermatol 14(3): 86-91.
- Asokan N, Prathap P, Ajithkumar K, Ambooken B, Binesh VG, et al. (2009) Pattern of skin diseases among patients attending a tertiary care teaching hospital in Kerala. Indian J Dermato Venereol Leprol 75: 517-518.
- Devi T, Zamzachin G (2006) Pattern of skin diseases in Imphal. Indian J Dermatol 51: 149-150.
- Aman S, Nadeem M, Mahmood K, Ghafoor MB (2017) Pattern of skin diseases among patients attending a tertiary care hospital in Lahore, Pakistan. Journal of Taibah University Medical Sciences 12(5): 392-396.
- Shah SK, Bjanushali DG, Sachdev A, Geria AN, Alexis AF (2011) A survey of skin conditions and concerns in South Asian Americans: A community based. Study. J Drugs Dermatol 10(5): 524-528.
- Evers AW, LU Y, Duller P, Vandervalk PG, Kraaimaat FW, et al. (2005) Common burden of chronic skin diseases? Contributors to psychological distress in adults with psoriasis and atopic dermatitis. British Journal of Dermatology 152(6): 1275-1281.
- Inanir I, Şahin MT, Gündüz K, Dinç G, Türel A, et al. (2002) Prevalence of skin conditions in primary school children in Turkey: differences based on socioeconomic factors. Pediatric dermatology 19(4): 307- 311.
- Bahamdan KA, Egeno JU, Khare AK, Tallab T, Ibrahim K, et al. (1995) The pattern of skin diseases in the Asir region,Saudia Arabia: A 12 month prospective study in a referral hospital. Ann Saudi Med 15: 455-457.
- Dayal SG, Gupta GD (1972) A cross section of skin diseases in Bundelkhand region, UP. Ind J Derm Ven Leprol 43: 258-261.
- Dogra S, Kumar B (2003) Epidemiology of skin diseases in school children; A study from Northern India pediatorpermatol 20(6): 470-473.
- Hossain MM (1993) Pattern of Skin and Sexually Transmitted Disease in District Hospital. Bangladesh J Dermatol Venerol Leprol 10(2): 7-9.
- Haque FM, Zaman AKB (2017) The Factors Affecting the Occurrence of Skin Diseases in Rajshahi, Bangladesh. Ijsrm Human 6(1): 63-71.
