 Case Report
Case ReportABSTRACT
Background: Lipomas are benign adipose tissue tumours, very common in
superficial locations. Deep-seated ones like those involving the gastrointestinal tract are
uncommon and involvement of the anal canal is rare. We present an incidental finding
of a submucosal lipoma of the anal canal in an elderly patient with colonic diverticulosis.
Case Presentation: A 70-year-old man was referred for colonoscopy on account
of recurrent passage of bloody stool of three months duration. There was no history
of anal protrusion, anal pain/discomfort, change in bowel habit, tenesmus, melaena
or abdominal pain. No history of fever or weight loss and he had no comorbid illness.
He was pale on examination, otherwise other aspects of his general and systemic
examinations were normal. At colonoscopy, he had multiple diverticuli in the caecum,
ascending colon and descending colon with a sessile polyp in the descending colon.
There was a yellowish, oval submucosal sessile mass with a lobulated surface, about
3cm from the anal verge and an increased yellowish hue to the large bowel submucosa
in the anal canal and at the sites of diverticula. The anal submucosal mass was biopsied.
Conclusion: Lipomas of the anal canal are rare. Although an incidental endoscopic
finding in this report, coexistence of large bowel lipomas with increased submucosal
adiposis colonic diverticuli may suggest an aetiological role of such lipomas in colonic
diverticulosis.
Keywords: Anal Lipoma; Endoscopy; Colonic Diverticulosis; Submucosal Adiposis
Background
Lipomas are benign adipose tissue tumors commoner between
the ages 40 -60 years and have a preponderance in the male gender
[1]. They may be solitary or multiple, superficial or deep in location
and are usually asymptomatic. Cosmetic concerns (in larger
lipomas), pain or discomfort are the common indications for removal
of superficial lipomas and these commonly occur in the trunk, head
and neck regions. Deep-seated lipomas are relatively uncommon;
they occur in the thorax, retroperitoneum or abdominal cavity [2].
Intra-abdominal lipomas usually affect the omentum, mesentery,
the submucosa and subserosa of the gastrointestinal tract (GIT) [3].
Lipomas are the second most common non-epithelial benign GIT
tumours after leiomyomas [4]. The most commonly affected region
of the GIT is the colon, with the highest incidence at the cecum, ascending colon, transverse colon, and the left colon (in decreasing
order as one approaches the rectum) [4]. Occurrence of a lipoma in
the anal canal is extremely rare with only one case reported so far
by Porta et al in 1979! [5].
In diverticulosis of the colon, there is a transmural outpouching
of the colonic mucosa through an area of weakness. This
mural weakness-the primary pathology in diverticulosis-is of
multifactorial aetiology and the predisposing factors include
weakened points of vascular entry into the colonic wall, reduced
dietary fiber, hereditary factor, reduced physical activity and
obesity [6]. In ventral abdominal wall hernias, stretching of
abdominal musculature (because of an increase in its content as
seen in obesity) and separation of muscle fibers with weakening
of aponeurosis are known to weaken the integrity of the fascia
leading to herniation [7]. Whilst the role of mural adipose tissue in
the development of GIT diverticula is yet to be established, Yekeler
et al have however reported a case of two coexisting rarities- an
oesophageal lipoma that resulted in an oesophageal diverticulum
due to extramucosal impact of the lipoma [8]. We present an
interesting incidental finding of a submucosal anal lipoma in an
elderly man who had a concomitant presence of colonic diverticula
with an increased submucosal adipose tissue in the vicinity of the
diverticuli. This case is reported in line with the SCARE criteria for
case reports [9].
Case Presentation
A 70-year-old male retiree was referred for colonoscopy
on account of recurrent passage of bloody stool of three months
duration, last episode being two weeks earlier. He had no history
of anal pain, discomfort, or anal protrusion. There was no change
in bowel habit, reduction in stool caliber, melaena, abdominal pain
or tenesmus. There was no history of anorexia, haematemesis,
early satiety and he does not have a history of peptic ulcer disease.
He had no fever, weight loss or any comorbid illness. He had no
history of anal trauma or previous anal surgery. No personal or
family history of similar illness or malignancy in the past. He was
not on any anticoagulation. On examination, he was pale, otherwise
other aspects of his general and systemic examinations were
normal with a body mass index of 23.1 kg/m2. A pre-procedural
rectal examination did not reveal any abnormality. Colonoscopy
revealed multiple diverticuli in the caecum, ascending colon and
descending colon (Figure 1a) with a 5mm x 3mm sessile polyp in
the descending colon.
There was a yellowish, oval, submucosal sessile mass (about
10mm x 8mm in widest diameters) with a lobulated surface, about
3cm from the anal verge (Figure 1b). The mass exhibited positive
pillow or cushion sign. The mucosa of the transverse colon, sigmoid
colon (Figure 1c) and rectum was normal. However, there was an
increased yellowish hue to the large bowel submucosa around the
anal canal (Figure 1d) and the sites of diverticula (Figure 1e). No
stigmata of recent bleeding were seen. The descending colonic
polyp was removed with cold biopsy forceps (Figure 2a). The anal
submucosal mass was biopsied revealing the characteristic naked
fat sign (Figure 2b). The anal submucosal mass was reported to
be benign at histology while the descending colonic polyp was
reported as an adenomatous polyp with low grade dysplasia. He
has been on conservative care for the colonic diverticulum and has
remained asymptomatic both for the diverticulum and the anal
submucosal lipoma 3 months post colonoscopy.
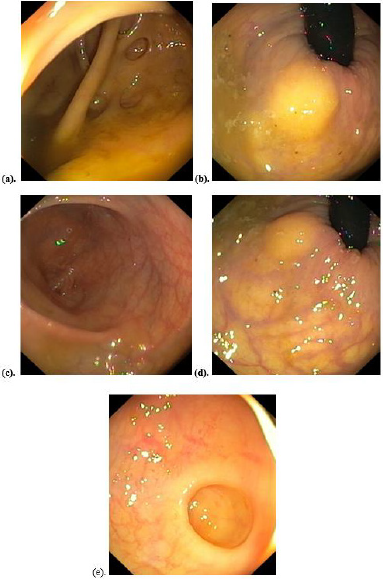
Figure 1: Colonoscopic findings:
a) Caecal diverticuli
b) Yellowish submucosal mass of the anal canal
c) Sigmoid colon mucosa
d) Increased submucosal adipose tissue around anal mass
e) Increased submucosal adipose tissue around a sigmoid colon diverticulum.
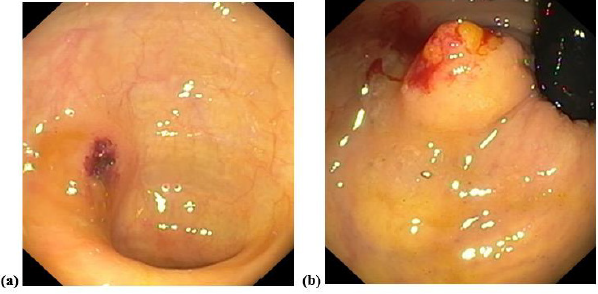
Figure 2:
a) Site of descending colonic polypectomy
b) Anal mass showing spilling out of adipose tissue following biopsy (naked fat sign).
Discussion
Lipomas are common benign tumour of mature adipose tissue
that usually occur in superficial locations – most common location
being subcutaneous. The relatively uncommon deep-seated
lipomas either present atypically or as incidental findings [10]. In
the GIT, they are usually subserosal or submucosal in location, the
colon being the most affected region. Involvement of the rest of
the large bowel decreases anal-ward. We presented an extremely
rare report of a submucosal lipoma of the anal canal with a curious
finding of concomitant existence of divertculi at areas of increased
submucosal adipose tissue. We discuss this case in terms of rarity
and then, its peculiarities. The rarity of this case lies in the fact that
it is a deep-seated lipoma occurring in the anal canal. The most
distal GIT lipomas reported in the literature are those of the rectum
and these presented as polypoid submucosal masses protruding
through the anal canal or casuing rectal bleeding [11,12]. Beyond
the rectoanal canal, the perianal region, lipomas are also rare with
a report of a perianal lipoma occurring years after surgery for a
perianal abdscess [13].
The aetiology of the perianal lipoma was likely traumatic,
similar to the report by Uscilowska et al on para-anal lipoma
resulting from perineal trauma [14]. Beyond trauma, the other risk factors for lipoma formation include genetic predisposition,
obesity, hyperlipidaemia and diabetes mellitus [15]. There risk
factor for lipoma in our patient was not apparent. This was not a
surprise since such deep-seated lipomas are incidentalomas like
in our patient. Colonic lipomas are usually asymptomatic except
when they are larger than 2cm, torsed, or pendulated. The small
size, submucosal location and sessile nature of the lipoma in our
patient may explain the asymptomatic nature. The sigmoid colon
is said to be the commonest site of colonic diverticulosis, although
a study on our patient population by Akere et al revealed right
colonic preponderance [16,17] The endoscopic appearance of
most colonic diverticuli is that of an outpouching of the mucosa
with an otherwise pink-looking mucosa/submucosa due to the
rich vasculature of these layers. In diverticulitis, the mucosa of the
diverticulum is reddened with or without a surrounding fibrinous
slough [18].
The peculiarity of our report is the increased submucoal
adiposis in the vicinity of colonic diverticuli, with a predominantly
yellowish (than pink) hue to the mucosal color (Figure 1e). These
diverticuli involved the caecum, ascending and descending colon
with none in the sigmoid colon, the mucosa of which appeared
normal (Figure 1c). It therefore stimulates curiosity as to a possible
link between increased large bowel mural adiposi and a possible
predisposition to subsequent diverticulum formation in the areas
where these adipose tissues are located. The plausibility of this
link may not be far-fetched if the underlying pathology of colonic
diverticulum- mural weakness-is considered. It is therefore more
compelling to associate increased submucosal adiposis in our
patient with his colonic diverticuli considering the established
effect of same adipose tissues on tougher tissues like aponeurosis in
abdominal wall hernias. Whilst colonic diverticulosis is commoner
in older patients like our patient, Brouland et al reported a large
colonic diverticulum in a young male arising due to colonic mural
weakness by multiple colonic lipomatosis [19].
The risk factors for colonic diverticulosis include comorbidities
(like hypertension and diabetes mellitus), increased luminal
pressure (from colonic dysmotility, reduced dietary fiber), genetic
risk factors (like Ehlers-Danlos syndrome, Coffin-Lowry and renal
polycystic disease), obesity/reduced physical activity, smoking
and increasing age [20]. Age alone may not explain the diverticuli
seen in our report and none of the other known risk factors was
apparent. Although the endoscopic features of the submucosal
anal mass we reported were in keeping with a lipoma, histological
report did not show the presence of adipocytes. This is a common
limitation of endoscopic biopsies where only the mucosal layer is
usually biopsied except multiple biopsies are taken at the same
spot to include deeper layers. A limitation of this report is our
inability to do endoscopic ultrasound which would have confirmed
the location of the lipoma. Facility for endoscopic ultrasound is not
available in Nigeria as at the time of this report to the best of our
understanding.
Conclusion
Lipomas of the anal canal are rare. Although an incidental endoscopic finding in this report, coexistence of large bowel lipomas with increased submucosal adiposis in the vicinity of colonic diverticuli may suggest an aetiological role of such lipomas in colonic diverticulosis.
Consent
A written informed consent was obtained from the patient to report this case.
Declaration of Interest
None.
References
- Emegoakor CD, Echezona CN, Onwukamuche ME, Nzeakor HO (2017) Giant lipomas: a report of two cases. Niger J Gen Pract 15: 46-49.
- Al-Ali MH, Salih AM, Ahmed OF, Kakamad FH, Mohammed SH, et al. (2019) Retroperitoneal lipoma: a benign condition with frightening presentation. Int J Case Rep 57: 63-66.
- Özer M, Ulusoy S, Parlak Ö (2016) A rare location: a giant mesenteric lipoma. Med J Islamic World Acad Sci 24(1): 24-26.
- Narindra rajaonarison ny ony L, Ahmad A, Bruneton J (2014) Lipomas of the digestive tract: General aspects and imaging. Cureus 6(9): e208.
- Porta E, Cazzaniga A (1979) Lipoma of the anal canal. Minerva Chir 34(22):1557-1560.
- Rezapour M, Ali S, Stollman N (2018)Diverticular disease: an update on pathogenesis and management. Gut Liver 12(2): 125-132.
- Dabbas N, Adams K, Pearson K, Royle GT (2011) Frequency of abdominal wall hernias: is classical teaching out of date? J R Soc Med Sh Rep 2(5): 1-6.
- Yekeler E, Yazicioglu A, Subasi M, Boztepe H (2016) Giant oesophageal lipoma as an uncommon cause of diverticula. Case Rep Gatsroenterol 10: 446-451.
- Agha RA, Borrelli MR, Farwana R, Koshy K, Fowler A, et al. (2018) The SCARE 2018 Statement: Updating Consensus Surgical CAse REport (SCARE) Guidelines. International Journal of Surgery 60: 132-136.
- Ulasi IB, Afuwape OO, Ajani MA, Onyema AE, Nwadiokwu JI, et al. (2021) A giant pre-peritoneal lipoma: a report of an uncommon presentation of a rare entity and a review of the literature. Surg Case Rep 4(7):1-5.
- Chakrabarti A, Goenka MK (2016) Submucosal lipoma of the rectum presenting as rectal prolapse and appearing as adenomatous polyp on confocal laser endomicroscopy, a case report and literature review. Gastroenterol Hepatol Open Access 5(1): 6-8.
- Bagherzade G, Etemad O (2017) Recto-sigmoid lipoma: a case report and review of the literature. J Coloproctol 37(1): 50-54.
- González-Urquijo M, Zambrano-Lara M, Espinosa-Loera JJ, Gil-Galindo G (2020) Perianal lipoma with an intersphincteric fistula in an adult patient. Rev Gastroenterol Mex (Engl Ed) 85(3): 368-370.
- Uscilowska E, Orabi NA, Leonard D, Mourin-Jouret A, Libbrecht L, et al. (2019) Para-anal lipoma as a rare consequence to perineal trauma: case report and review of the literature. Acta Chir Belg 119(6): 390-395.
- Guler O, Mutlu S, Mahirogullari M (2015) Giant lipoma of the back affecting quality of life. Ann Med Surg 4: 279-282.
- Perry AF, Keku TO, Martin CF, Eluri S, Runge T, et al. (2016) Distribution and Characteristics of Colonic Diverticula in a United States Screening Population. Clin Gastroenterol Hepatol 14(7): 980-985.
- Akere A, Ogoh GS, Tejan E (2017) Clinical presentation of patients and distribution of colonic diverticula during colonoscopy at a tertiary hospital in south-west Nigeria. Trop J Health Sci 24(1): 8-12.
- Gross M, Labenz J, Börsch G, Dormann A, Eckardt AJ, et al. (2015) Colonoscopy in acute diverticulitis. Viszeralmedizin 31:124-129.
- Brouland J, Poupard B, Nemeth J, Valleur P (2000) Lipomatous polyposis of the colon with multiple lipomas of the peritoneal folds and giant diverticulosis: report of a case. Dis Colon Rectum 43(12): 1767-1769.
- Violi A, Cambie G, Miraglia C, Barchi A, Nouvenne A, et al. (2018)Epidemiology and risk factors for diverticular disease. Acta Biomed 89(9):107-112.
