 Research Article
Research ArticleABSTRACT
Introduction: Goiter is a condition characterized by enlargement of the thyroid gland by the time one reaches puberty. Several genetic and environmental factors contribute to thyroid disease. Thyroid gland enlargement is frequently observed in clinical practice as a result of iodine deficiency, an increase in TSH levels, natural goitrogen, smoking, and insufficient selenium and iron. These conditions are usually associated with either hypothyroidism or hyperthyroidism, or with elevated TSH levels. Objective: The main purpose of the study was to determine the frequency of goiter in the lower Dir population and categorize it on the basis of age, gender, size and visibility.
Methods: In the descriptive cross-sectional retrospective study, 405 patients were included between July 2020 and June 2021. Individual data including occupation, ethnicity, gender, age, residential area, economic status, physical appearance of the goiter, and status of education were collected using a structured questionnaire. In accordance with WHO guidelines, goiters were assessed for each subject.
Results: The difference between goiter prevalence in the sexes is well documented, with a higher frequency in women. The study concluded that the prevalence of goiter was overwhelmingly higher in women (n=247/61.0%) than in men (n=158/39.0%) and among people with grade 2 visible goiter was relatively high (n=176/43.5%). A subgroup analysis revealed that many patients (n=272/67.2%) were not aware of goiter, and also that the number of illiterate people (n=267/65.7%) was higher than literate people (n=138/34.1%).
Conclusion: The study area has a high prevalence of goiter, so the health sector should increase community awareness of iodized salt and foods rich in iodine through disseminating key messages about these foods.
Keywords: Goiter; TSH; District Lower Dir; Iodine Deficiency
Introduction
The thyroid gland is responsible for producing thyroid hormone, which has an important role in metabolic processes. It is essential for these hormones to have adequate amounts of iodine [1,2]. Goiter can be detected clinically by palpation and physical examination when there are insufficient amounts of iodine [3,4]. In several areas of the world, goiter is considered a significant problem for public health, especially in developing countries, and is an indicator of chronic iodine deficiency [5]. Iodine deficiency disorders (IDDs) affect 30% of the population globally. There are more than 150 million IDD patients worldwide [6]. Thyroid nodules and goiters are the most common thyroid conditions due to a combination of genetic, environmental, and endogenous factors [7]. Around 15.8% of the general population develop goiter, and iodine is a significant environmental factor that influences goiter prevalence [7]. A thyroid nodule can be detected by ultrasound in 19% to 67% of cases, but only 4–7% is palpable [8]. Most thyroid nodules and goiters do not present any symptoms; however, they can be associated with other disorders, including endocrine dysfunction, impaired body composition, autoimmune thyroid disease and various metabolic disorders [9]. Coordinating basal metabolic rate and thermogenesis is a key role for thyroid hormones [10].
Researchers have linked low thyroid hormone levels with poor metabolic health in several studies, even when they are within normal limits. There are many metabolic processes regulated by thyroid hormone, including growth and development, reproduction, and enhancing metabolism [11]. The thyroid produces and releases thyroxine (T4) and triiodothyronine (T3) into the circulation system. Thyroid stimulating hormone (TSH) is released by the anterior pituitary gland and helps to regulate thyroid hormone levels, which are controlled by thyrotropin releasing hormone (TRH) from the hypothalamus. A negative feedback loop is present between TRH and TSH in the circulation system, and the regulation is carried out by T4 and T3 [12,13]. An iodine deficiency causes goiter, the enlarged thyroid glands that are greater than the terminal phalanx of the thumb, which indicates chronic iodine deficiency [14].
Goiters provide an indication of the iodine status in a region and can be used as a long-term indicator of the success of an iodine programmer. A measurement of the prevalence of goiter caused by iodine deficiency is based on indicators like urinary iodine concentrations (UIC) and total goiter prevalence (TGP) as well as the proportion of salt in households that is adequately iodized (>15 ppm) [15]. Throughout the world, iodine deficiency is the leading cause of goiter [16-18]. Iodine deficiency was reported in Pakistan by the World Health Organization in 1990 as affecting an estimated 50 million people; goiter was reported as prevalent as 80-90% in mountainous areas [19]. Cretinism is estimated to have a prevalence of about 3% in the general population [20]. Lower Dir District is situated in Malakand Division of Khyber Pakhtunkhwa province in Pakistan. There are 1.05 million people living in Timergara City, the district capital and largest city with 1,582 square kilometers. Our main objective in this study was to find out the prevalence and factors of goiter in hospitalized patients residing in District Timergara, Dir Lower Pakistan.
Methods
Study Setting, Design, and Participants
A descriptive cross-sectional retrospective study of hospitalized patients was conducted from July 2020 to June 2021 in District Timergara, Dir Lower Pakistan. There were 405 participants in the study (247 women and 158 men). The study comprised all patients admitted to the endocrinology department at the (DHQ) Timergara hospital regardless of the reason for admission. Throughout the examination, every patient’s clinical history was examined, as well as the previous case record. We collected the information using a questionnaire designed to inquire about patients’ general socio-demographic data, including goiter physical appearance, age, occupation, ethnicity, gender, residential area, economic status, educational, and clinical manifestations, among other considerations, are considered. A trained endocrine specialist, who has already examined the patients, written informed consent was obtained from all participants. In the study, patients with serious physical and mental illnesses were excluded as it was difficult to obtain data and measurements from them. The study was approved by the Ethical Committee of the Department of Surgical, Institute of Paramedical Sciences Khyber Medical University Pakistan, which followed the recommendations of the Declaration of Government District Headquarter Hospital (DHQ) of Timergara, Dir Lower.
Examination for Goiter
Using palpation techniques, a trained and experienced public health officer assessed the presence of goiters based on WHO/ UNICEF/ICCIDD criteria [21]. Therefore, Grade 0: stand for not visible, not palpable; Grade: I stand for palpable, not visible; and Grade: II stands for visible and palpable.
Statistical Analysis
In order to examine the data, the patient’s records were manually checked, sorted, categorized, and coded. Then, SPSS version 23.0 was used to analyze the results. We measured the prevalence of goiter based on the relative frequencies and ratios for all patients with goiter.
Results
In total, 405 patients were recruited to participate in this study. Here are the sociodemographics characteristics of the participants (Table 1). Out of the 405 respondents, 247 were women (61.0%) and 158 were men (39.0%), and goiter was much more prevalent in women than in men. All of the patients were of the same ethnicity, patients with no formal education had the highest prevalence of goiter, 267 (65.9%), and 138 (34.1%) patients were literate. As educated levels increased, goiter prevalence declined, reaching the lowest levels in comparison to illiterate patients. The results revealed that 278 (68.6%) were married and 127 (31.4%) were unmarried, while 129 (31.9%) were government employees, and that most of the patients were farmers with no proper job 267 (68.1%). Participants were sorted by age into 10-year age groups based on the results the prevalence of goiter was lowest among those between the ages of 14-24 (10.4%), while among 35–44-yearolds, the rate reaches its highest level (37.5%). Goiter prevalence was greater in hilly than plain areas, at 283 (69.9%) in hilly and 122 (30.1%) in plain. In hilly areas, goiter was significantly more prevalent than in plain areas. On the basis of thyroid examination, there were 176 (43.5%) patients with palpable and visible goiter (grade II), and goiter prevalence was higher in individuals aged 35- 44 years old (37.5%) (Figure 1).
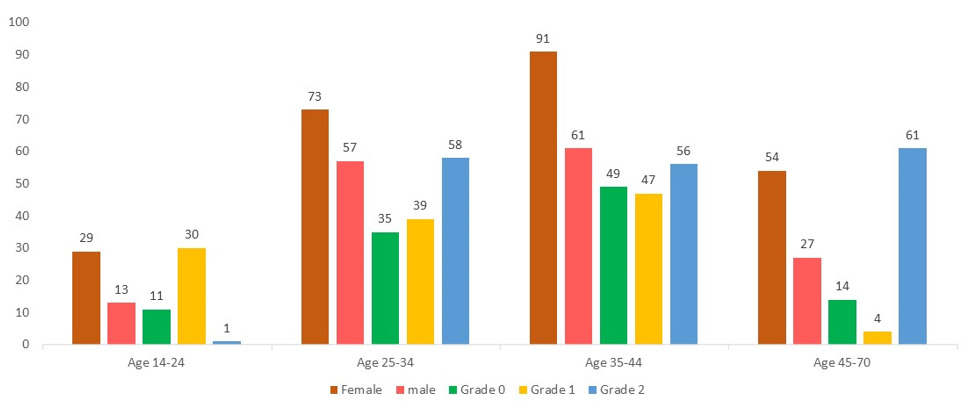
Figure 1: Age and gender-wise prevalence of goiter among hospitalized patients.
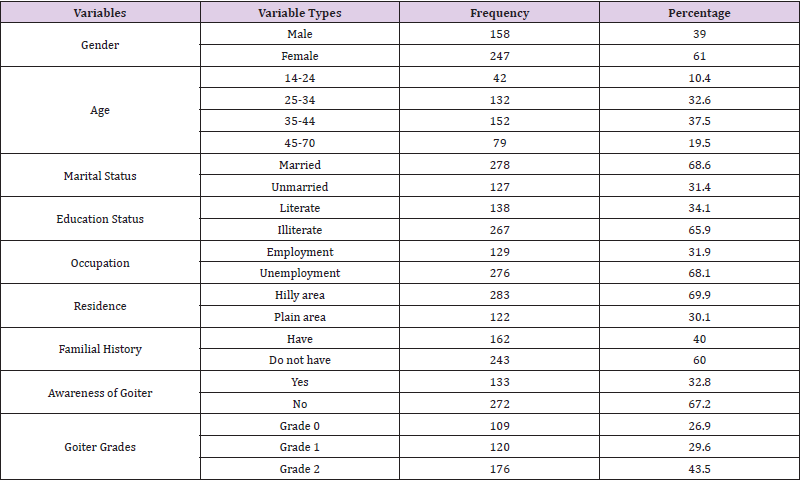
Table 1: Sociodemographics characteristics of goiter hospitalized patients.
Discussion
Goiter is a common endocrine problem that affects around 300 million people globally, with more than half of those affected being unaware of their condition. The most common thyroid disorders are hyperthyroidism and hypothyroidism, which affect 1.6 billion people in more than 100 countries around the world [22-27]. Our findings revealed that females were more prone to goiter than males, as demonstrated by their ratio of (61.0%) to (39.0%), although overall goiter prevalence did not significantly differ between genders. During this study, goiter cases were classified according to age, with older patients 35-44 (37.5 %) having a higher prevalence than younger patients. There is a documented association between the prevalence of goiters and gender. Interestingly, Knudsen et al. observed that men were more likely to have goiters than women; however, women were two to ten times more likely than men to have goiters [28,29]. Studies have shown that sex hormones may play a role in thyroid volume only after puberty, suggesting that changes in thyroid volume are influenced by gender differences [30]. In addition, women are more likely than men to develop thyroid problems during their lifetime [31,32]. There was a study that found older women had a higher risk of goiter than younger women. A higher prevalence of goiter was observed with age in areas with severe or moderate to mild iodine deficiency. Other studies report an enlargement of the thyroid gland with age in areas with severe or moderate iodine deficiency [33].
According to this study, goiter was most prevalent in illiterate patients compared to literate patients because illiterate individuals were unaware of goiter. The findings of our study are in agreement with previous research findings, which found that the prevalence of goiter increased in hilly areas in comparison to plain areas. Goiter is more prevalent in Baltistan, Northeast Pakistan, where the prevalence was found to be 16.6% among the general population. In the North, it is 20.4% of males, 28.1% of females, and the South 13.9% of males, 21.2% of females [34]. In previous studies, it was discovered that northern Pakistan has become one of the first known areas to have an iodine deficiency. Goiters have been reported in only a few studies across various regions of Pakistan, ranging from the Northern region in the upper Himalaya to the lower Himalaya and even on the Punjab plains. It was estimated in 1990 that 70% of the population was at the risk of iodine deficiency related disorder, with the prevalence of goiters ranging from 55% in plains to 80-90% in the northern mountainous region [35]. According to the WHO classification of goiter based on size and visibility, 7 percent of the global population possesses visible form goiter [36], our results showed that the prevalence of goiter on the basis of thyroid examination with palpable and visible (grade II) was high frequency 176 (43.5 %), the goiter rate was higher in the 35-44 years of age group (37.5%). The prevalence of goiter was reported to be 3.4 % in women and 6.9 % in men among French citizens [37], 23.9 and 35.6 % in German citizens, 58.1 % in Italian citizens [38] and 35.7 % in Romanian citizens [38]. According to Hatemi et al., the prevalence of goiters using neck palpation was 30.5% in Turkey [39]. However, the prevalence was higher than the 16 % and 27 % reported by a report about global iodine deficiency in world and African populations [40]. Similarly, the prevalence of goiter in Ethiopia was higher than various studies which showed a prevalence ranging from 26.3% to 62.1% among children [41-44]. The main cause of goiter is iodine deficiency, and it is imperative to concentrate prevention efforts at the society level on eliminating iodine deficiencies.
Conclusion
The study conclusions suggest that goiter prevalence might depend on TSH levels specific to normal or abnormal hormonal dysfunction. The study also concluded that increased goiter risk was independently related to women’s gender and low TSH levels. The study area had an iodine deficiency problem, and goiter was linked to increased parity, older age, and illiteracy. The study area has a high prevalence of goiter. The health sector of the district should invest more efforts in spreading important messages about iodized salt and iodine-rich foods to ensure community awareness. There is a need for a systematic investigation of the epidemiological profile of patients with diffuse goiter. It is necessary to conduct further research on both the environmental and genetic interactions that lead to goiter.
Acknowledgment
Thanks are given to the people in the endocrinology department at the Department of Health and Welfare (DHQ) Health Department Timergara, as well as the health extension workers, study participants, and questionnaire translators.
Authors’ Contribution
Research was initiated, written, conducted, and analyzed by NA. IU, IH, and SA were involved in writing the proposal, interpreting the data, and writing the manuscript. The final manuscript has been read and approved by all authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors’ Contributions:
Research was initiated, written, conducted, and analyzed by Irfan Ullah, Naqash Alam, Muhammad Asif, Ihtisham Ul Haq, Sadiq Ali were involved in writing the proposal, interpreting the data, and writing the manuscript.
References
- Antonio C Bianco, Grant Anderson, Douglas Forrest, Valerie Anne Galton, Balázs Gereben, et al. (2014) American Thyroid Association Guide to Investigating Thyroid Hormone Economy and Action in Rodent and Cell Models. Thyroid 24(1): 88-168.
- Cheng S Y, Leonard J L, Davis P J (2010) Molecular aspects of thyroid hormone actions. Endocrine reviews 31(2): 139-170.
- Zimmermann M B (2011) The role of iodine in human growth and development. In Seminars in cell & developmental biology 22(6): 645-652.
- (2020) World Health Organization United Nations Children’s Fund, International Council for Control of Iodine Deficiency Disorders. Assessment of iodine deficiency disorders and monitoring their elimination. A guide for programme managers.
- (2007) World Health Organization. United Nations Children’s Fund, International Council for the Control of Iodine Deficiency Disorders 2007 Assessment of iodine deficiency disorders and monitoring their elimination. Geneva, Switzerland: World Health Organization, p. 14-16.
- (2014) World Health Organization. Goitre as a determinant of the prevalence and severity of iodine deficiency disorders in populations (No. WHO/NMH/NHD/EPG/14.5). World Health Organization.
- Andersson M, Takkouche B, Egli I, Allen H E, Benoist BD, et al. (2005) Current global iodine status and progress over the last decade towards the elimination of iodine deficiency. Bulletin of the World Health Organization 83(7): 518-525.
- Dauksiene D, Petkeviciene J, Klumbiene J, Verkauskiene R, Vainikonyte-Kristapone J, et al. (2017) Factors associated with the prevalence of thyroid nodules and goiter in middle-aged euthyroid subjects. International journal of endocrinology 2017.
- Zheng L, Yan W, Kong Y, Liang P, Mu Y, et al. (2015) An epidemiological study of risk factors of thyroid nodule and goiter in Chinese women. International journal of environmental research and public health 12(9): 11608-11620.
- Laurberg P, Knudsen N, Andersen S, Carlé A, Pedersen I B, et al. (2012) Thyroid function and obesity. European thyroid journal 1(3): 159-167.
- Roef G L, Rietzschel E R, Van Daele C M, Taes Y E, De Buyzere M L, et al. (2014) Triiodothyronine and free thyroxine levels are differentially associated with metabolic profile and adiposity-related cardiovascular risk markers in euthyroid middle-aged subjects. Thyroid 24(2): 223-231.
- In: Conn P M, Melmed S (Eds.)., (1997) Endocrinology: Basic and clinical principles. Springer Science & Business Media.
- Pataueg A, Larson E T, Brown C L (2021) Evolution of Thyroid Enhancement of Embryogenesis and Early Survival.
- Abuye C, Berhane Y, Ersumo T (2008) The role of changing diet and altitude on goitre prevalence in five regional states in Ethiopia. East Afr J Public Health 5(3): 163-168.
- Torheim L E, Granli G I, Sidibé C S, Traoré A K, Oshaug A, et al. (2005) Women's iodine status and its determinants in an iodine-deficient area in the Kayes region, Mali. Public health nutrition 8(4): 387-394.
- (1990) WHO. Report to the 43rd World Health Assembly. Geneva: World Health Organization.
- Delange F (1994) The disorders induced by iodine deficiency. Thyroid 4(1): 107-128.
- De Benoist B, Andersson M, Egli I, Takkouche B, Allen H, et al. (2004) Iodine status worldwide: WHO global database on iodine deficiency. Geneva: World Health Organization.
- Ghayur S (2001) Spectrum of iodine deficiency in school children of Rawalpindi, Pak. Armed Forces Med J 51(1): 27-32.
- Chapman J A, Grant I S, Taylor G, Mahmud K, Ul-Mulk S, et al. (1972) Endemic goitre in the Gilgit agency, west Pakistan. Philosophical Transactions of the Royal Society of London. B, Biological Sciences, 263(856): 459-490.
- Saira S, Khattak R M, Rehman A U, Khan A A, Khattak M N K, et al. (2014) Prevalence of goiter and iodine status in 6-12 years school children and pregnant women of district charsadda, pakistan. Acta Endocrinologica (1841-0987) 10(1): 65-75.
- Rafiq M (1996) Iodine deficiency disorders program in Pakistan (An analytical review). University of Leeds.
- Hussain I, Soofi S B, Hasan S, Mehboob N, Hussain M, et al. (2013) Impact on health and nutrition outcomes in Sindh province, Pakistan. IDS Bulletin 44(3): 38-47.
- Azizi F (2002) Assesment monitoring and evaluation of iodine deficiency disorders in the middle east and eastern mediterranian region. Sara.
- Kazi A, Qureshi M (1998) A critical analysis of nutritional studies in Pakistan (1956-1985) Part II: malnutrition mortality and related deficiencies. Pak J Med Res 37(3): 132-43.
- Muktar M, Roba K T, Mengistie B, Gebremichael B, Tessema A B, et al. (2019) Goiter and its associated factors among primary school children aged 6-12 years in Anchar district, Eastern Ethiopia. PloS one 14(4): e0214927.
- Abdullaeva M, Kasimova G, Yaxudayev E, Sakhibova M, Bakhavadinova Z, et al. (2020) The Influence of Dysfunction of the Autonomic System and the Thyroid Gland on the Course of Bronchial Asthma (BA) in Children. Int J Cur Res Rev 12(14): 36.
- Haymart M R, Repplinger D J, Leverson G E, Elson DF, Sippel R S, et al. (2008) Higher serum thyroid stimulating hormone level in thyroid nodule patients is associated with greater risks of differentiated thyroid cancer and advanced tumor stage. The Journal of Clinical Endocrinology & Metabolism 93(3): 809-814.
- Knudsen N, BuÈlow I, Jørgensen T, Laurberg P, Ovesen L, et al. (2000) Goitre prevalence and thyroid abnormalities at ultrasonography: a comparative epidemiological study in two regions with slightly different iodine status. Clinical endocrinology 53(4): 479-485.
- Rapoport B, Chazenbalk G D, Jaume J C, McLachlan S M (1998) The thyrotropin (TSH)-releasing hormone receptor: interaction with TSH and autoantibodies. Endocrine reviews 19(6): 673-716.
- Wiersinga W M (2013) Smoking and thyroid. Clinical endocrinology 79(2): 145-151.
- Bukhari U, Sadiq S (2008) Histopathological audit of goiter: A study of 998 thyroid lesions. Pakistan Journal of Medical Sciences 24(3): 442.
- Adesunkanmi A R K, Makinde O N (2003) Goitre prevalence in pregnant women attending antenatal clinic in a teaching hospital. Journal of Obstetrics and Gynaecology 23(2): 156-159.
- Derumeaux H, Valeix P, Castetbon K, Bensimon M, Boutron-Ruault MC, et al. (2003) Association of selenium with thyroid volume and echostructure in 35-to 60-year-old French adults. European Journal of Endocrinology 148(3): 309-315.
- Farahati J, Wegscheider K, Christ K, Gilman E, Oing W, et al. (2006) Gender-specific determinants of goiter. Biological trace element research 113(3): 223-230.
- Aghini-Lombardi F, Antonangeli L, Martino E, Vitti P, Maccherini D, et al. (1999) The spectrum of thyroid disorders in an iodine-deficient community: the Pescopagano survey. The Journal of Clinical Endocrinology & Metabolism 84(2): 561-566.
- Simescu M (1991) Study on the evolution of endemic goiter in Romania. Endocrinologie, 29(1-2): 73-83.
- Erdoğan G (2005) Kologlu Basic and Clinical Endocrinology. Second edition. Nobel Medical Publications, Ankara, pp. 525-544.
- Mesele M, Degu G, Gebrehiwot H (2014) Prevalence and associated factors of goiter among rural children aged 6-12 years old in Northwest Ethiopia, cross-sectional study. BMC public health 14(1): 1-8.
- Yadav N K, Thanpari C, Shrewastwa M K, Sathian B, Mittal R K, et al. (2013) Socio demographic wise risk assessment of thyroid function abnormalities in far western region of Nepal: A hospital based descriptive study. Asian pacific journal of tropical disease 3(2): 150-154.
- Andersson M, Takkouche B, Egli I, Allen H E, Benoist B D, et al. (2005) Current global iodine status and progress over the last decade towards the elimination of iodine deficiency. Bulletin of the World Health Organization 83(7): 518-525.
- Qamar M F, Abbas S (2012) Prevalence and case reports of goiter at district Bahawalpur, Pakistan. Science International (Lahore) 24(1): 1013-5316.
- Enyew H D, Zemedkun K G, Dagnaw A M (2015) Prevalence of goiter and associated factors among primary school children aged 6–12 years old in GobaTown, South East, Ethiopia. Int J Nutr Food Sci 4(3): 381-387.
- Gebriel T W, Assegid S, Assefa H (2014) Cross-sectional survey of goiter prevalence and household salt iodization levels in Assosa Town, Beni Shangul-Gumuz Region, West Ethiopia. J Preg Child Health 1(119): 2.
