 Case Report
Case ReportABSTRACT
Introduction: Surgical treatment of clavicle fractures is becoming more frequent as it reduces the nonunion rate, shortens the time to union and also provides better esthetic outcomes. Acute postoperative pain is moderate to severe, so planning for adequate perioperative pain management is essential.
Case Description: A 32-year-old man suffered an isolated right middle third clavicle fracture after a motorcycle traffic accident. He was proposed for osteosynthesis with autologous bone graft harvested from the iliac crest. As part of the anesthetic plan, the patient underwent general anesthesia combined with clavipectoral fascia block, superficial cervical plexus block and transverse plane abdominal (TAP) block. The postoperative analgesic regimen was maintained with intravenous analgesia, reporting pain VAS (visual analogue score) <2. The patient did not present any complications during the first 48 hours after surgery and was discharged home uneventfully.
Conclusion: Combined general anesthesia with clavipectoral fascia block, superficial cervical block and transversus abdominis plane block is an excellent alternative for patients undergoing clavicular fracture osteosynthesis, being an easy and effective regional anesthesia method when performed under ultrasound guidance and providing excellent intra and postoperative analgesia of long duration.
Introduction
Surgical treatment of clavicle fractures is becoming more frequent as it reduces the nonunion rate, shortens the time to union and also provides better esthetic outcomes [1]. Acute postoperative pain is moderate to severe requiring opioids for its´ management, so planning for adequate perioperative pain management is essential. Clavicle surgery is usually performed under general anesthesia combined with interscalene plexus block, where phrenic nerve paralysis can reach up to 70% [2] depending on the technique which can be a relevant unwanted effect in patients with pulmonary disease, obesity or with concomitant rib fractures as in polytrauma [3]. We describe a novel anesthesia management of this fracture which has been made possible by advances in the use of ultrasound for guidance of locoregional anesthesia.
Case Description
A 32-year-old man suffered an isolated right middle third clavicle fracture after a motorcycle accident. He was proposed for osteosynthesis with autologous bone graft harvested from the iliac crest (Figure 1). The patient had no relevant past personal medical history, ASA physical status I, weight 75 kg. As part of the anesthetic plan, the patient underwent general anesthesia (intravenous induction: Fentanyl 200 mcg + Propofol 200mg + Rocuronium 50 mg; maintainance: Sevoflurane in O2/air) combined with ultrasound-guided locoregional anesthesia performed after general anesthesia was established: clavipectoral fascia block (Ropivacaine 0.5% 10ml 50mg), superficial cervical plexus block (Ropivacaine 0.5% 10ml 50mg) and transverse plane abdominal (TAP) block (Ropivacaine 0.5% 20ml 100mg). No intraoperative complications occurred and the patient was extubated immediately at the end of the procedure. He did not require any intraoperative opioids after general anesthesia induction nor during the postoperative period. The postoperative analgesic regimen was mantained with intravenous Paracetamol 50 mg q 8 hours alternating with Dexketoprofen 50mg q 8 hours, achieving pain VAS (visual analogue score) <2. The patient was discharged home uneventfully after 48 hours (Figure 2).
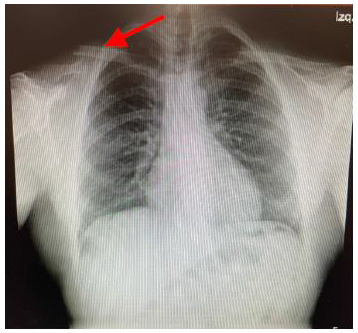
Figure 1: Preoperative x-ray where the fracture is seen.

Figure 2: Postoperative radiographic control illustrating satisfactory osteosynthesis.
Discussion
While the cutaneous innervation of the skin above the clavicle is supplied by the supraclavicular nerve of the superficial cervical plexus, the sensory innervation of the clavicle is complex and unclear [4], it seems to be provided by terminal branches of the braquial plexus such as subclavian, long thoracic and suprascapular nerves, passing through the plane between fascia and clavicle [5]. The combination of interscalene plexus block and superficial cervical plexus block reach a good level of postoperative analgesia for clavicle fractures. However, supplementation with intraoperative opioids is necessary because the skin and medial clavicle sensory innervation is not blocked. Also, various side effects have been described, the most relevant being phrenic nerve paralysis. In this context, the clavipectoral block is a good alternative for pain management being an easy and safe technique when performed with ultrasound guidance.
Clavipectoral block was described by Valdes- Vilches in 2017. The clavipectoral fascia covers the clavicular site of the pectoralis major muscle. Compared with interscalene plexus block, clavipectoral fascia block offers a more lateral and superficial plane, far from neurovascular structures, the clavicle being a natural backstop during injection. When properly done, no specific adverse effects of this technique have been described [3]. The literature on the clavipectoral plexus block combined with deep cervical plexus block being used as a single anesthetic modality for surgery of the clavicle is scarce [3]. Combining it with superficial cervical plexus block is beneficial for providing analgesia of the skin incision. In this case, it was necessary to harvest bone graft from the iliac crest. There is high incidence of severe postoperative pain (39%) [6] with this procedure. The TAP block is a good solution for pain control. Regional anesthesia results in less overall opiod consumption decreasing nausea, vomiting and possible hyperalgesia and immunodepressive effects [7]. It enables early deambulation and patient discharge.
Technique
Clavipectoral fascia block: in supine position, the superficial cervical plexus was blocked. Then the linear transducer probe (11 MHz) was placed on the anterior surface of the medial third of the clavicle. A 20-gauge block needle (35 mm) was inserted in a caudal to cephalic direction. An injection of local anesthetic under ultrasound guidance was made between the clavipectoral fascia and the periosteum on the medial and lateral area of clavicle injury [5] (Figure 3). The TAP block was performed in supine position, with a 22-gauge block needle (80 mm), the injection of local anesthetic was made between the internal oblique muscle and transversus abdominis muscle.
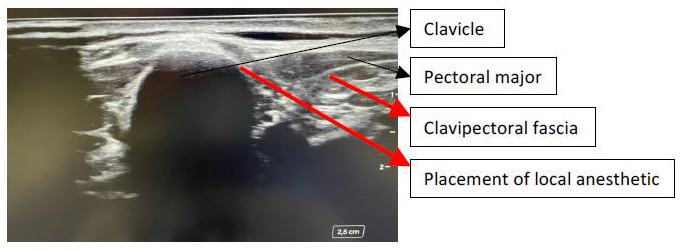
Figure 3: Ultrasound landmarks to identify clavipectoral fascia.
Conclusion
Combined general anesthesia with clavipectoral fascia block and deep cervical block is an excellent alternative for patients undergoing clavicular fracture surgery, being a successful and effective regional anesthesia method. We present it as an alternative to interscalene brachial plexus block, eliminating intra and postoperative opioid consumption and possible phrenic nerve paralysis. This case illustrates the efficacy of clavipectoral fascial block as a peripheral nerve block in clavicle surgery. Additional studies are required in order to clarify the anatomy, innervation and distribution of the sensory blockade and the efficacy and safety of the clavipectoral block in this context.
References
- Balaban O, Dülgeroğlu TC, Aydın T (2018) Ultrasound-Guided Combined Interscalene-Cervical Plexus Block for Surgical Anesthesia in Clavicular Fractures: A Retrospective Observational Study. Anesthesiol Res Pract 3: 7842128.
- Verelst P, Van Zundert A (2013) Respiratory impact of analgesic strategies for shoulder surgery. Reg Anesth Pain Med 38(1): 50-53.
- Kukreja P, Davis CJ, MacBeth L, Feinstein J, Kalagara H (2020) Ultrasound-Guided Clavipectoral Fascial Plane Block for Surgery Involving the Clavicle: A Case Series. Cureus 12(7): e9072.
- Valdés-Vilches L (2017) Analgesia for clavicular surgery/fractures. In Symposia 01: Postoperative analgesia for Orthopedic upper and lower limb surgery. Symposium conducted at the 36th Annual European Society of Regional Anaesthesia and Pain Therapy (ESRA) Congress, Lugano, Switzerland.
- Ince I, Kilicaslan A, Roques V, Elsharkawy H, Valdes L (2019) Ultrasound-guided clavipectoral fascial plane block in a patient undergoing clavicular surgery. J Clin Anesth 58: 125-127.
- Chin KJ, Chan V, Hebbard P, Tan JS, Harris M, et al. (2012) Ultrasound-guided transversalis fascia plane block provides analgesia for anterior iliac crest bone graft harvesting. Can J Anaesth 59(1): 122-123.
- Bugada D, Lorini LF, Lavand'homme P (2021) Opioid free anesthesia: evidence for short and long-term outcome. Minerva Anestesiol 87(2): 230-237.
