 Mini Review
Mini ReviewABSTRACT
This paper presents an innovation of a curved alveolar bone distractor used mainly to augment defects in the anterior regions of the dental arch. It is designed to be a bone anchored distractor and the working components of the distractor are exposed in the oral cavity to the facial side for easy access. The selective rotation of the translator nut pushes the traction bracket to move the movable bony segment in increments following the path of the curved activation rod thus augmenting the defect in a manner conforming to the contour of the natural dental arch. The present distractor has the advantages over the available distractors in the market in that it is a bone anchored distractor that augment the anterior alveolar defects in a curved shape similar to the contour of the dental arch.
Keywords: Distraction Osteogenesis; Distractor Device; Curved Anterior Arch Distractor; Augmentation of Anterior Alveolar Defect
Introduction
The novel device presented is related to oral and maxillofacial instruments [1], particularly curved distractors for oral and maxillofacial reconstruction, which offer improved anatomical conformity for reconstruction, easy access for regular adjustments, and light weight for convenience of use and ease of manufacture (Figures 1 & 2). Commonly used surgical procedures for anterior alveolar defects, such as cleft alveolar defect repairs, require bone augmentation for esthetic and functional requirements to furnish a foundation for the completion of dental reconstructions, such as dental implants. However, some patients do not possess the requisite physiological foundation of soft and hard tissues for reconstruction the shape of the dental arch to facilitate dental implants placement. Typically, the oral anatomy of one patient differs from another to varying degrees. Distraction Osteogenesis (DO) is a procedure that remedies such deficiencies by inducing additional or new bone and soft tissue growth at the deficient target area [2-5].
A typical DO procedure augments bone and soft tissues by transecting a bone segment adjacent to the target area using a distractor device that maintains a preselected separation between the transected sections and transfers gradually the aimed sectioned bone segment towards the opposing side of the bone defect with the activation of the distractor by preferably 1 mm each day [6]. The distractor is incrementally activated over time until the desired separation and induced growth is attained in the distracted area.
Materials and Methods
Description of the Distractor
The presented curved distractor permits necessary adjustments to accommodate the specific anatomy of a patient’ dental arch. (Figure 1) illustrates components of the presented distractor and example of its use for augmenting a defect in an anterior upper alveolar defect. (Figure 2) shows a prototype of the curved alveolar distractor fixed on a model of a phantom upper dental arch illustrating the application of the distractor on an anterior defect site. The curved alveolar bone distractor includes an elongated curved and threaded traction rod supported on opposite ends by anchor brackets. The anchor brackets fix the traction rod onto the bony foundation of a patient’s jaw. The endcaps cap the opposite ends of the traction rod to prevent dislodging and define the extent of the working length of the traction rod. A traction bracket freely slides along the traction rod, while the traction bracket is fixed to a movable bony segment. A translator nut is threaded onto the traction rod to abut against the side of the traction bracket. The curved shape of the traction rod ensures that the distraction occurs along a curvilinear path such that the new bone and tissue growth conforms more to the natural contours of the patient’s jaw.
The selective rotation of the translator nut pushes the traction bracket to move the movable bony segment at a predetermined distraction distance. When assembled and installed, the working components of the curved distractor are exposed in the oral cavity to the facial side for easy access. Tools were provided to operate the translator nut. The proposed anterior alveolar bone defect is aimed to gain a new bone matching the curvature of the dental arch. A targeted and sectioned bone segment in one side of the defect was distracted through the curvature of the curved activating rod towards the opposing side conforming the curvature of the dental arch (Figures 1 & 2).
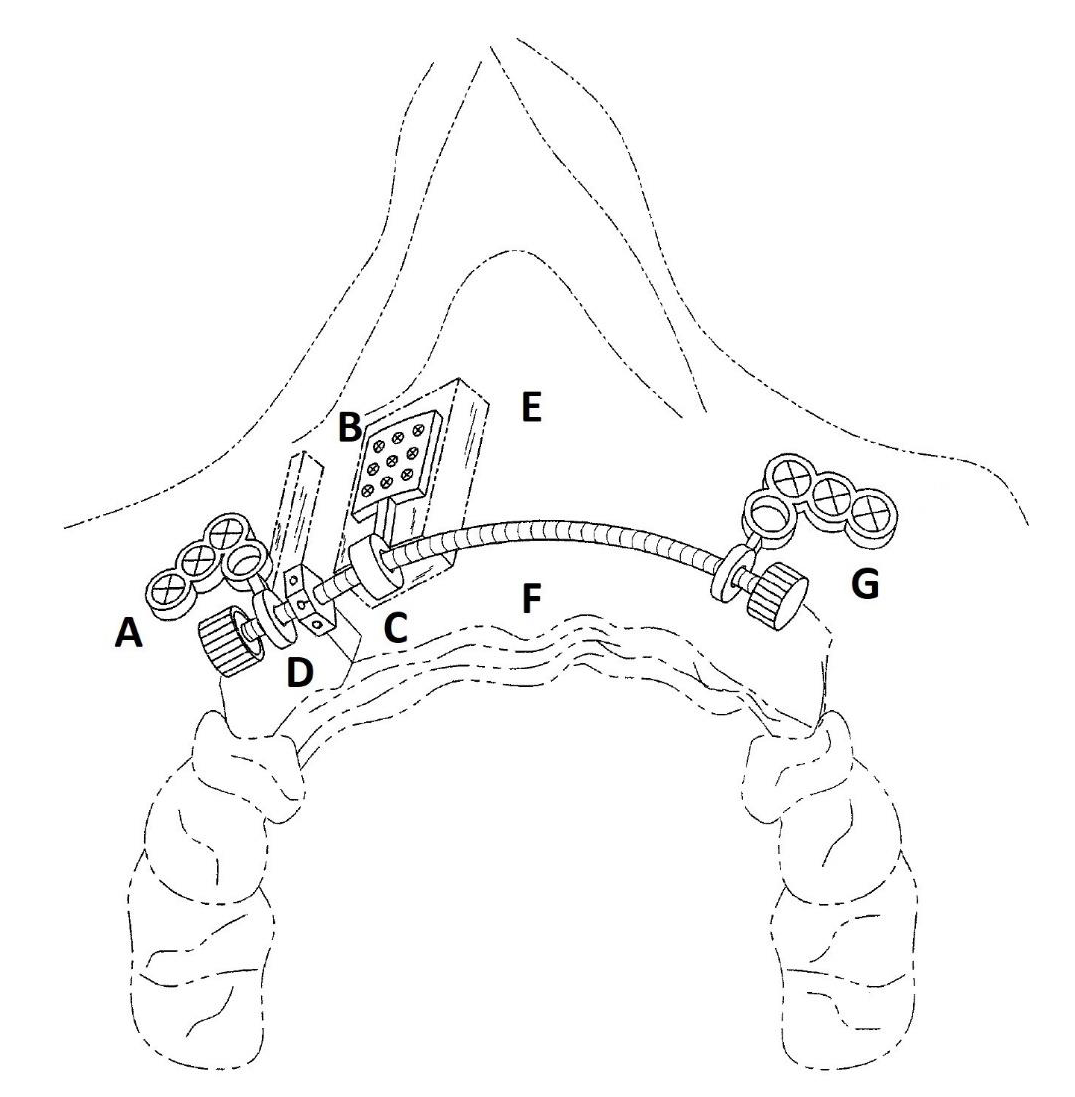
Figure 1:
A. Is a perspective view of the curved distractor device in the patient mouth. The anchor plates is fastened with mini- screws to the alveolar bone at both sides of the defect in the maxilla.
B. The moving bone segment is fastened to the mesh plate with mini-screws.
C. Its bracket is attached to the curved activation distraction bar.
D. The translator nut.
E. Is placed left to the sectioned bone segment.
F. Pushing the bone segment in increments during its rotation allowing gradual movement of the bone segment towards the other side of the maxilla following the curved path of the distraction bar.
G. Note a pair of first and second endcaps threaded onto the ends of the traction rod to prevent dislodging of the distractor components.
Surgical Procedure
The following is an example of a surgical procedure. Under local anesthesia, the labial mucoperiosteum of the alveolar bone on both sides of the defect was surgically exposed together with the labial mucoperiosteum of the bony segment that was preselected as the freely moving part. The freely moving bony segment was separated from the adjacent fixed bony part by a surgical saw starting labial until it reached palatal. The traction bracket was adapted to the labial surface of the freely moving bony segment, for example, by trimming and/or shaping the mesh plate or shaping the mounting ring as necessary. The traction bar passed through the mounting ring with the mesh plate in place. The translator nut was threaded onto the traction rod from the side of the surgically created bony cut line mesial to the mounting ring and distal to the anchor bracket. The translator nut was assembled between the anchor brackets and adjacent to the mounting ring. The ends of the traction rod were inserted through the mounting rings in a passive manner the anchor plates were then shaped by bending to conform or adapt to the surfaces of the non-moving bone at both sides of the defect before fixing the anchor plates and mesh plate.

Figure 2: Shows photographs of prototype of the curved alveolar distractor fixed on a phantom model of upper dental arch illustrating the application of the distractor on a defect site at the premaxilla.
A. The proposed alveolar bone defect gained new bone matching the curvature of the dental arch by distracting an aimed sectioned bone segment in one side of the defect
B. distract it through the curvilinear of the curved activating rod towards the opposing side.
The traction rod was supported by the mounting rings during adaptation of the anchor plates and mesh plate. The anchor plates were then fixed with fasteners, such as self-drilling screws, on the labial surface of the non-moving parts of the jaw. Subsequently, several fasteners were used to fix the mesh plate to the labial surface of the moving bony segment. After fixing the anchor plates and mesh plate, the freely moving bony segment was completely separated from the adjacent fixed bony surfaces at the surgical bony cut line using a small chisel. After verifying the stability of all components of the curved distractor, the endcaps were tightened to the ends of the traction rod. The translator nut was rotated using a wrench or pinlever provided with the surgical kit for approximately two counterclockwise revolutions, equating to a distance of approximately 1 mm. This process verifies the action of the curved distractor and the smooth traction of the freely moving bony segment. The soft tissue layers were sutured back, and the distraction process was then commenced at a typically recommended rate of 1 mm per day until the targeted distraction distance was reached. When the distraction process and healing duration is complete, the curved distractor may be easily disassembled and removed with minor surgery.
Discussion
Distracting the hard and soft tissues to augment alveolar defect in in the anterior dental cannot be by any means result in an ideal aesthetic contour and functional bone foundation to reconstruct dental missing teeth by using the straight distractor devices. Currently used distractors to augment anterior alveolar maxillary and mandibular defects are typically constrained to distract the bone in a straight line or are dependent on tooth bearing [2, 3] tend to be heavy owing to their relatively large components, not stable as they depend on their weak anchors attached to the adjacent teeth and may be designed with components submerged under the submucosal layers. These factors may lead to a final reconstruction that does not comply with the correct curvature of the jaw arch, patient discomfort, losing of their components in the dental anchored dependent distractors or unforeseen complications as their components covered by the soft tissue layers. Difficulties in solving problems with the distractor bar activation and difficulties in performing adjustments may also arise from the submerged portions of the typical distractor owing to limited accessibility. Moreover, the area for reconstruction may not follow a curvilinear line.
To this end, a curved alveolar bone distractor that solves the aforementioned problems is presented in this paper. The exposed Curved distractor components permits necessary adjustments to accommodate the specific anatomy of a patient. The bone anchored distractor ensures that distraction process and the distracted bone segment moves with stability. Thus, the curved distractor serves as a relatively simple, convenient, and easy-to-use device for distraction. The curved shape of the traction rod ensures that the induced growth of new bone and tissue follows a curvilinear path that closely matches the contours of the patient’s jaw. The working components of the curved distractor, such as the traction rod and translator nut, are exposed to the facial side of the patient’s mouth so that they can easily be accessed by the oral surgeon for periodic adjustments of the distraction distance. Moreover, the components of the curved distractor are constructed from relatively lightweight materials, which substantially reduces potential discomfort and complications for the patient.
Acknowledgment
Author would like to thank the College of Dentistry Research Center and Deanship of Scientific Research at King Saud Saud University, Saudi Arabia for funding this research project (research project FR0600).
References
- Al ruhaimi K (2017) Curved alveolar bone distractor. US Patent 9,622,782; BL Publishing.
- Hegab AF (2012) Closure of the alveolar cleft by bone segment transport using an intraoral tooth-borne custom made distraction device. J Oral Maxillofac Surg 70(5): 337-348.
- Erverdi N, Küçükkeleş N, Şener C, Selamet BU (2012) Interdental distraction osteogenesis for the management of alveolar clefts: Archwise distraction. Int J Oral Maxillofac Surg 41(1): 37-41.
- Choi SH, Park JH, Cha JY, Jung HD (2019) Intraoral premaxillary distraction in a patient with maxillary retrognathic cleft lip and palate: A case report. Cleft Palate Craniofac J 56(6): 827-830.
- Sung Hwan Choi, Jin Hoo Park, Jung Yul Cha, Hwi Dong Jung (2003) Use of distraction osteogenesis in cleft palate patients. Angle Orthod 73(5): 602-607.
- Al ruhaimi KA (2001) Comparison of different distraction rates in the mandible: An experimental investigation. Int J Oral Maxillofac Surg 30(3): 220-227.
