 Research Article
Research ArticleSUMMARY
In this article authors discussed results of investigation of 106 patients with delay of puberty in age 11-16 years old. They noted that these patients have hypogonadotropic hypogonadism (HH). In all age periods of puberty by Tanner patients have low mean levels of LH, FSH, and total testosterone with some hyperprolactinemia. It was diagnosed 3 degrees of severity of HH: easy (11,3%), middle (16,04%) and hard (72,6%).
Keywords: Delay of Puberty; Teenagers
Background
Negative medical and demographic trends, which are noted in the past 15 years in the CIS, are closely interrelated with progressive deterioration in the reproductive health of the population [1-4]. As is known, the delay in sexual development or pubertata implies the lack of an increase in the testicular volume (<4 ml) and if the length of the testicles does not reach 2.5 cm (<4 ml) at the age of 15 [5]. In accordance with the ICD-10, the delay of sexual development is highlighted as an independent endocrine disease. PD (Puberty delay, or somatosexual development) is one of the actual problems of endocrinology, andrology and sexopathology, attracting the attention of specialists from various centers. According to various authors, the frequency of the PD ranges from 0.4% to 9.8%, and over the past decades it is noted [6,7]. The differential diagnosis of the isolated deficiency of gonadotropic hormones and the constitutional delay of sexual development is the necessary and difficult task in the daily work of the endocrinologist. Since the clinical picture with these states is similar, it is quite difficult to distinguish them. Therefore, the study of the hormonal profile is an urgent diagnostic procedure [5].
For an isolated shortage of gonadotropic hormones, a normal growth and normal growth rate is characterized, and for the constitutional delay of sexual development is characterized by lowness. In both states, the basal levels of LH and FSH are reduced, and the levels of other pituitary hormones are within the normal range. Therefore, ordinary hormonal studies and sample with gonadoliberin are not given anything for a diagnosis. With a constitutional delay in sexual development, the basal level of prolactin is normal or slightly reduced and significantly increases after the administration of Tyrolyberin. In the majority of patients with an isolated shortage of gonadotropic hormones, the basal level of prolactin is low and does not increase either slightly increase after stimulation by Tyrolyiberin [8]. Hypogonadism, in contrast to the delay of sexual development, which can be viewed as a border state, is a disease with a serious disorder of the functioning of the entire reproductive system requiring a long (sometimes constant) hormonal therapy.
Often, parents (sometimes children themselves) are addressed to the doctors - pediatricians, therapists, urologists, endocrinologists (sometimes children) with complaints about the lagging in the development of genital organs regarding peers. Some of these patients are sent to the consultation by other specialists. In about 90% of cases, as a result of the survey, it turns out that the delay in sexual development in a child (adolescent, young men) is absent. However, the overwhelming majority of doctors in solving these issues only focus on the subjective perception of the somatic status of the patient and their practical experience. Meanwhile, it is necessary to objectify anamnesis, inspection, the results of a laboratory survey to obtain reliable results regardless of personal experience and the subjective opinion of the doctor. All the above appeared the basis for this study.
The Purpose of the Study
The purpose of the study is to study hormonal disorders in adolescents (boys)with hypogonadotropic hypogonadism in sexual development stages. Material and research methods. 523 pupils of schools of Nukus and 4 districts had detailed examination of 143 adolescents aged from 11 to 16 years have been examined. From the examined patients, we found 106 (20.3%) adolescents aged 11-16 years, suffering from the delay of pubertate to varying degrees. All 106 patients were performed by a study spectrum, which included the study of endocrine status, generally clinical, biochemical, hormonal (STS, LH, FSH, Prolactin, TSH, testosterone, cortisol, free thyroxine, etc.), in addition, anthropometric studies were performed to all adolescents (target height, centile, growth rate, SDS growth and weight, etc.) based on the international growth-weight map of Tanner-Weithaus, estimates of the penal development stage on a tanner (using tables and an orchidometer), if necessary - X-ray (radiograph of brush and Turkish saddle , radiography brushes, ultrasound of the thyroid gland and genital organs. The data of control of the appropriate age and gender for hormonal studies were provided by the Hormonal Research Laboratory of the Center of Endocrinology of PHM of RUz. The data obtained was processed using Microsoft Excel and Statistica_6 computer programs. The differences between the groups were considered statistically significant at Р< 0.05. The average values (m) were calculated, standard deviations of medium (M).
Results
Table 1 is given the distribution of patients by age. As can be seen from Table 1, most often among the examined patients aged 13.2 ± 0.8 years and 15.5 ± 0.7 years (36.7% and 30.1%) were met. Table 2 shows the average values of various hormones in patients with PD in sexual development stages. Table 2 it follows that in all age-related periods of sexual development, the surveyed patients had hypogonadotropic hypogonadism (HH): a significant decrease in the average levels of LH, FSH, a total testosterone - from (p <0.05) was noted. In this case, the lowest these values were in patients with 2 Puberty stages, that is, aged 11.7 ± 1.3 years (n = 17) on the background of normoprolactinemia. The average levels of prolactin were not reliably elevated in patients 3 and 5 of the stages of the Tanner (P> 0.05). It should be emphasized that the levels of STHs, TSH and free thyroxine, as well as cortisol, were within the norm in all patients (N = 106). When comparing the stages of pubertate and hormonal data, it was revealed that as the ages increases, the average values of LH, FSH, a common testosterone, although they remain reliably reduced. Next, we analyzed cases of the lowest values of LH, FSH and the total testosterone, namely, when the LH/ FSH levels ranged from 0.1 to 0.9 IU/L, from - from 1 to 3 nmol / l (severe degree of HH) , cases of average gonadotropin values and from when the levels of LH/FSH were ranging from 1 to 4 IU/L, from - from 3 to 7 nmol / l (average severity of the HH), as well as cases with a slight degree of GG, when levels LH/FSH ranged from 4 and above, from - from 7 nmol/ l and higher (easy severity of HH).
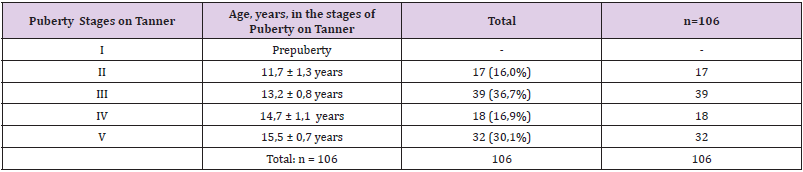
Table 1: The distribution of patients by age. (5 Tanner Stages).
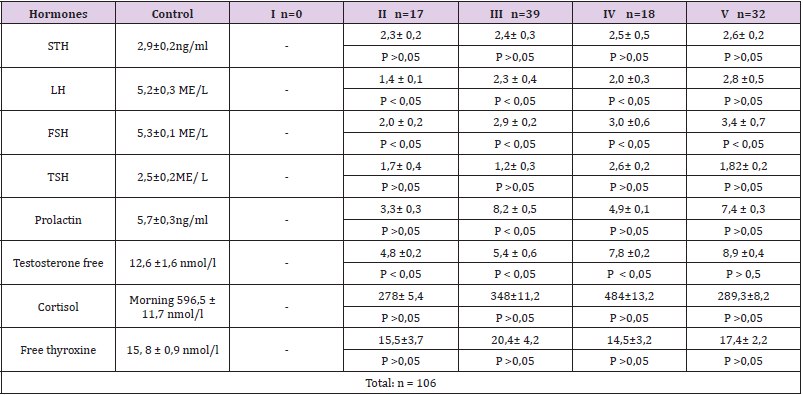
Table 2: Average values of hormones in patients according 5 Tanner stages.
Note: Р – The accuracy of differences compared to the control group. In the table for comparison, there are vibrations of hormone levels from 11 to 16 years of control group (healthy faces).
Thus, this characteristic allowed us to highlight 3 groups of patients with 3 degrees of gravity HH - moderately, medium and heavy - depending on the mean values of LH, FSH, from. These data are shown in Tables 3-5. Table 3 shows the number of patients with a severe degree of Tanner’s stages. The total number of these patients turned out to be -39 (36.7%). As can be seen from the data in Table 3, when analyzing the lowest values of LH, FSH and the total testosterone, namely, when the LH / FSH levels ranged from 0.1 to 0.9 IU / L, from - from 1 to 3 nmol / l (severe degree of HH) The total number of cases was equal to 17 (16.04%). In this group, the reliability of differences was the highest (p <0.05). Table 4 shows the number of patients with the average degree of Tanner’s stages. The total number of these patients turned out to be 77 (72.6%). When analyzing the cases of moderate severity of the HH, we proceeded from those mean values of gonadotropins and from when the levels of LH/FSH were ranging from 1 to 4 m/ l, from - from 3 to 7 nmol/ l (average severity of the HH). In total, such cases turned out to be 77 (72.6%) and this group was dominant (p <0.05, as well as p> 0.05).
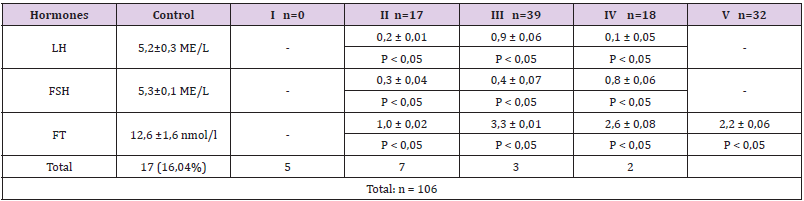
Table 3: The number of patients with a severe degree of HH, depending on the mean values of the LH, FSH and from the patients on 5 Tanner stages.
Note: FT- Free Testosterone., P is the accuracy of differences compared with control (1).
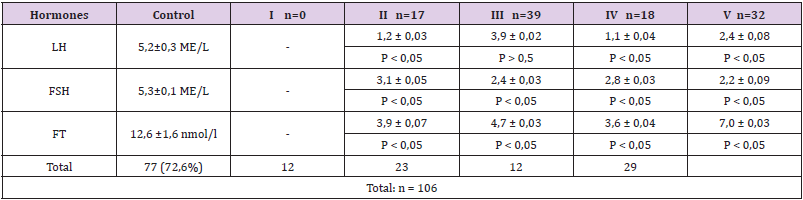
Table 4: The number of patients with the average severity of the HH, depending on the mean values of the LH, FSH and from the patients with 5 Tanner stages).
Note: FT- Free Testosterone., P is the accuracy of differences compared with control (1)
Table 5 is given the number of patients with a slight degree of HH in Tanner Stages. The total number of these patients turned out to be 12 (11.3%). Cases with a light degree of HH, when the LH / FSH levels were fluidated from 4 and above, from - from 7 nmol / l and above (an easy severity of HH) amounted to 12 patients (11.3%). In this group of patients, the reliability of differences in the content of LH, FSH, from plasma was less reliable, while in the range from p <0.05 to p> 0.05. Thus, the analysis of hormonal results showed that the average severity of the HH (72.6%) was most often observed, while less frequently met (16.04%) and light (11.3%) of its degree. Only 1 (0.9%) of the patient identified hypergronadotropic hypogonadism.
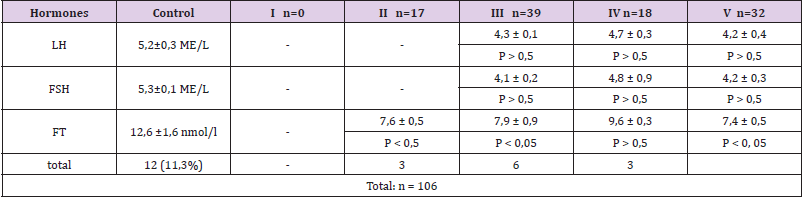
Table 5: The number of patients with a slight degree of HH, depending on the average values of the LH, FSH and from. Patients in 5 Tanner Stages).
Note: FT- Free Testosterone., P is the accuracy of differences compared with control (1)
Conclusion
1. In all age-related periods of sexual development, hypogonadotropic hypogonadism took place in the surveyed patients: a significant decrease in the average levels of LH, FSH, a total testosterone (p <0.05) was noted. Only 1 (0.9%) of the patient identified hypergronadotropic hypogonadism.
2. When comparing the stages of pubertate and hormonal data, it was revealed that as the ages increases, the average values of LH, FSH, the total testosterone, although they remain reliably reduced.
3. There are 3 severities of hypogonadotropic hypogonadism: light (11.3%), average (16.04%) and heavy (72.6%).
4. This category of patients’ needs further examination (magnetic resonance imaging of pituitary glands, ultrasound genital organs, etc.) and treatment [5].
References
- Bozted VA, OV Teodorovich (2005) Clinical epidemiology of male infertility. Sat. Materials of the II All-Russian Conference "Male Health", Moscow, p. 39.
- Kiryanov AV, S Yu Kalinchenko (2003) Delay of sexual development in boys. Andrology and Genital Surgery 2: 20-29.
- Ter-Avaneov GV, TA Nazarenko, VI Kulakov (2000) Fertility of men in the XXI century. Andrology and Genital Surgery 1: 32.
- Edouard T, Tauber M (2010) Delayed Puberty. Arch Pediatr 17(2): 195-200.
- Abdurahmanova AM (2011) The standards of hormones for the persons of the Uzbek population depending on the floor of the age. Methodical manual, Tashkent, p. 30.
- Baranov AA, V Yu Albitsky (2003) Social and organizational problems of pediatrics. M.: ID Dynasty, pp. 512.
- (2000) Informational letter "Protection of reproductive health of boys and young men - adolescents". Family planning 2: 10-15.
- Mirsky VE, St. Petersburg (1998) Scientific substantiation of the system of organization of specialized andraological assistance to children in a major city: author. dish. ... Cand. honey. Science, p. 25.
