 Research Article
Research ArticleABSTRACT
Background: Globally, pneumonia is the leading cause of mortality among children. Among high burden countries, Ethiopia ranks fifth. Regardless of this fact, efforts to identify determinants of pneumonia have been limited in the study area. Objective: Identify the determinants of community-acquired pneumonia among under-five children.
Methods: Institution-based unmatched case-control prospective study was carried out among 143 cases and 285 controls of under-five children. The data were collected using a structured and pre-tested questionnaire, then entered into Epi-info version 7 and analyzed using SPSS) version 20. logistic regression model was used to determine the effect of various factors on the outcome variable.
Results: The result of this study identified maternal age less than 25 years (AOR=3.98, 95% CI=2.16,7.31), family size greater than 4 (AOR=4.99, 95% CI=2.62,9.50),nonexclusive breast feeding (AOR=2.40, 95% CI=1.03,5.57), stunting (AOR=1.99, 95% CI=1.11, 3.60), history of diarrhea in the last 15 days (AOR=2.37,95% CI=1.13,4.98), charcoal used as a source of cooking fuel (AOR=6.09, 95% CI=2.77,17.12), lack of separate kitchen (AOR=2.20,95% CI=1.24, 3.91) and parental smoking (AOR=3.79, 95% CI=1.82, 7.90) were determinants of community acquired pneumonia among 2-59 month age children.
Conclusion: Maternal age< 25 years, family size> 4, non-exclusive breastfeeding, stunting, history of diarrhea, charcoal use as cooking fuel, and parental smoking were risk factors of community-acquired pneumonia. Limiting the family size, nutritional intervention, prevention and early treatment of diarrheal diseases, and preventing indoor air pollution could be optional interventions to reduce the risk of communityacquired pneumonia.
Keywords: Two-59-Month-Old Children; Pneumonia; Determinants
Abbreviations: CAP: Community Acquired Pneumonia; ICCM: Integrated Community Case Management; IMNCI: Integrated Management of Neonatal and Childhood Illness; UNICEF: United Nations International Children’s Emergency Fund; URTI: Upper Respiratory Tract In-
Introduction
Pneumonia is the inflammation of the lungs including the functional unit of the lung and bronchioles. Depending on the etiologic agent, it can be classified as infectious like bacterial, viral, fungal, parasitic, or non-infectious like aspiration of gastric contents or food [1-4]. Globally, about 156 million under-five children get affected by pneumonia each year and among this, about 151 million are in developing countries. Nearly 74% of cases of pneumonia are reported annually from fifteen countries [2]. Accordingly, Southeast Asia and Africa account for 39% and 30% of the global burden of community-acquired pneumonia respectively [5]. The estimated annual cases of pneumonia among under-five children in Ethiopia was 3,370,000 [6]. Deaths due to childhood pneumonia were above 0.9 million worldwide [7,8]. Among these deaths, more than 99% were in low and middle-income countries [9,10]. South Asia and sub-Saharan Africa bear the burden of more than half of the total number of cases of pneumonia among under-five children worldwide [5,11]. Pneumonia takes the lives of over 40,000 underfive children every year in Ethiopia, which is about 20% of all causes of death every year and the leading cause of death in the postnatal period [6,12,13]. Ethiopia ranks fifth having 62 deaths per 1000 live birth among the fifteen countries of high burden pneumonia cases [6]. In addition to health burden, pneumonia has a tremendous burden on the health system, the economy of the household, and the nation as a whole; the mean medical expenditure per outpatient visit for community-acquired pneumonia is US$8, and that for inpatient care of severe pneumonia is US$64 in Ethiopia as shown in a study [14].
Ethiopia adopted and implemented the WHO recommendation for classification and management of pneumonia since 2011 [15,16]. With the help from the economic support of its donors, United Nations International Children’s Emergency Fund (UNICEF) has guided the expansion of the Health Extension Program (HEP) and Integrated Community Case Management (ICCM) program and sets technical assistance to Ethiopia’s ministry of health [17]. Therefore, IMNCI and ICCM are currently functional pneumonia control strategies being implemented in the Ethiopian health center and health post levels respectively [18,19]. Although the implementation of affordable and effective interventions has reduced the burden of pneumonia, the progress has been uneven and the high level of pneumonia stress and trauma continued in many countries [20,21]. Even if the ICCM program saves thousands of young lives every year, pneumonia remains one of the common causes of child death and hospitalization in Ethiopia, and respiratory health problems are the most important reason for seeking health services [6,22- 25]. Research to identify the potential determinants of communityacquired pneumonia is required for planning proper prevention and control strategies. Even though there are studies conducted in different regions of Ethiopia, little is known about the determinants of community-acquired pneumonia among under-five children in the study area [26-29]. Therefore, this study is intended to assess determinants of community-ac pneumonia among 2–59-month age children attending health facilities in Hosanna Town.
Methods and Materials
Study Period and Area
This study was conducted from February 1, 2018, to May 15, 2019, among 2–59-month children who attended health facilities in Hossaena town, Hadiya zone, SNNPR, Ethiopia. The town is located 232 kilometers southwest of Addis Ababa, the capital city of Ethiopia, and 194 kilometers south of the regional city Hawassa. For a total of 92,733 populations, the town has one zonal public hospital, one private hospital, three health centers, and 26 private clinics. All of the public health facilities in Hossaena town provide services for an average of 170 under-five children every month, and 22 % of them are pneumonia cases. The entire public health facilities use the revised WHO IMNCI guideline protocol to classify and treat cases such as pneumonia, diarrhea, and fever. To assess and treat malnourished children, they use the acute malnutrition manual prepared by the Ethiopian federal ministry of Health. They also have organized immunization programs for infants, growth monitoring services, and vitamin A supplementation every six months for under-five children.
Study Design
An institution-based unmatched case-control study was conducted among 2–59-month children attended health facility in Hossaena town, SNNPR, Ethiopia.
Population
Source Population: All 2-59 months old children who attended public health facility in Hossaena town during the study period and their guardians/caregivers.
Study Population: Selected children aged 2-59 months who attended the selected health facilities during the study period and their guardians/caregivers.
Case: Children 2-59 months old who visited the under-five clinic, classified and registered for CAP as defined by revised WHO (IMCI) guideline during the data collection period.
Control: Children 2-59 months old who visited the under-five clinic, classified and registered for other conditions other than CAP as defined by revised WHO (IMCI) guidelines during the data collection period.
Inclusion and Exclusion Criteria
Inclusion Criteria: Children 2-59 months old who have pneumonia as defined by revised WHO (IMNCI) guideline was included as the case. Healthy 2-59 months old children or children with non-respiratory complaints as well as those who attended for immunization, growth monitoring, and wound care due to trauma or dermal infection were included as a control.
Exclusion Criteria: Children with the finding of asthma, congenital diseases, and other medical infection with respiratory complaints were excluded from this study.
Sample Size Determination: The sample size was calculated by two population proportion formulas using Epi info 7 STAT CALC program by taking assumption of 95 % confidence level, 80 % power, and 1:2 case-control ratio. The required final sample size for this particular study was obtained by taking the maximum number from the sample size calculation results see (Table 1) above and 10 % added for non-response rate which was 428 (143 cases and 285 control) children.
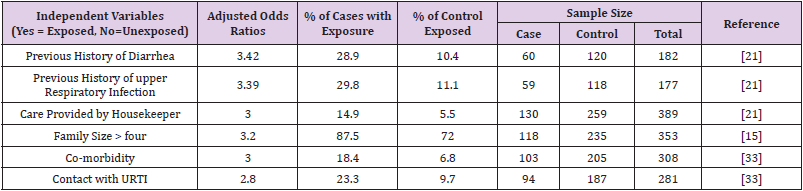
Table 1: Sample size determination for a study on determinants of community acquired pneumonia among 2-59 months age children attended health facility in Hossana town, SNNPR, Ethiopia, 2019.
Sampling Technique and Procedure: The entire health facilities in Hossaena town that provide services for under-five children as Integrated Management of Neonatal and Childhood Illness (IMNCI) protocol were included in this study. The sample sizes were proportionally distributed to each health facility based on Health Management Information System (HMIS) report of existing case and control flow in the previous three months (see Figure 1). Total sample size decided for this study as case and control were multiplied by case and control flow in each health facility in the previous three months divided by total case or control flow in all selected health facilities. Systematic sampling technique with the interval of three (456/143 =3) was used to select cases and controls.
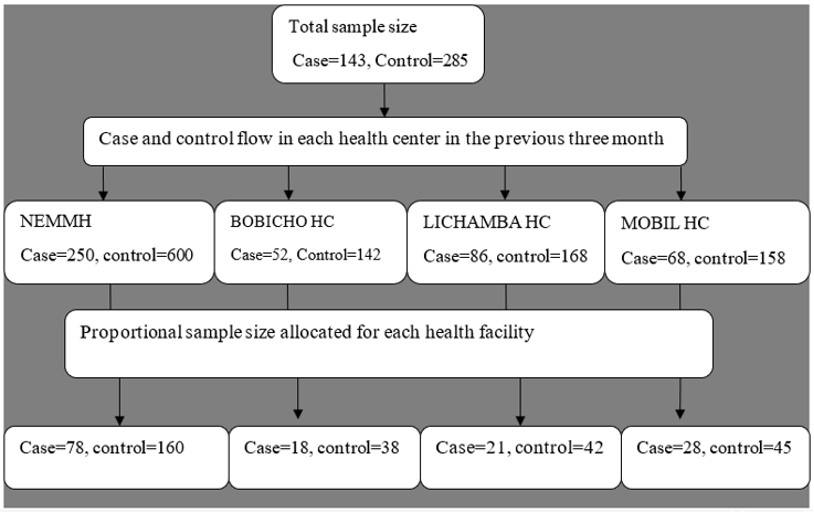
Note: NEMMMH=Nigist Eleni Mohammed Memorial Hospital. HC= Health Center
Figure 1: Proportional sample size allocation for a study on determinants of community acquired pneumonia among 2-59 months age children attending health facility in Hossaena town, SNNPR, Ethiopia, 2019.
Data Collection Tools and Procedures
Questionnaires were adapted from different literatures and translated in to Amharic and Hadiyisa languages and back translated to English language by language experts to check the consistency. The questionnaire is based on the possible risk factors of CAP including socio-demographic factors, nutritional and health status of the children and environmental factors. It was checked for consistency by back-translation to English; unclear and incomplete questionnaires were returned and completed [27,30- 32]. Before data collection informed consent was taken from all of the children parents. Data were collected by using structured and pretested interviewer administered questionnaires by eight trend nurses working in under-five clinic, and three health officers were assigned for supervision. Document review was done to select cases and controls. After the study subjects were identified as case and controls, they were sent to separate rooms with data collector; one for cases and the other for control. Afterwards, face to face interview with the parent or guardian based on interviewer administered questionnaire was done. To assess nutritional status of the children, Anthropometric measurements of weight to the nearest 0.1 gram by Salter scale using basin, length or height to the nearest 0.1 centimeter for under two and over-two-year children respectively by using stadiometer were measured.
Operational Definitions
(Table 2).
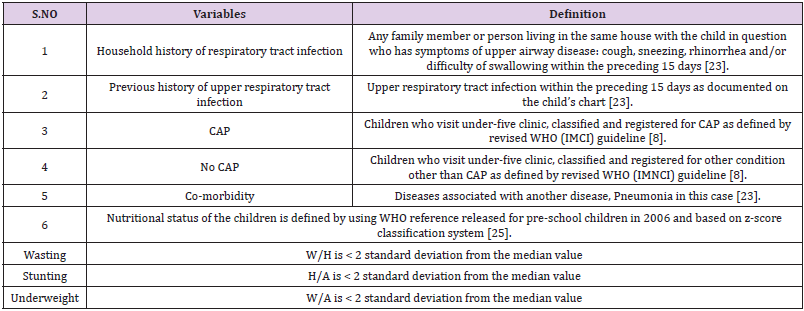
Table 2: Operational definitions of terms.
Data Entry and Analysis
Data were checked for completeness, edited, coded and entered in to Epi info 7 Software and exported to SPSS (version 20) for cleaning and analysis. The WHO anthro version 3.2.2 software was used for analysis of nutrition indexes to prepare for SPSS.WHO growth reference (2006) was used to report anthropometric result; Individual anthropometric data were compared with reference values on a graph using sex and age specific z-score classification system. Data were cleaned by running frequency, and by sorting reported variables. Different statistical assumptions, model fitness and multi-collinearity were checked and the appropriate correction mechanisms prior to data analysis were implemented. Both descriptive and inferential statistical techniques were employed. Mean, standard deviation, frequency and percentages were obtained for variables and odds ratios with 95% confidence interval were calculated. A binary logistic regression analysis was used to test the association between each independent variable with outcome variables. The variables showing statistically significant association with the out-come variable (up to p-value equal to 0.25) during binary logistic regression analysis were set as candidate and simultaneously included in multivariable logistic regression analysis. Finally, the variables with statistically significant associations at p-value less than 0.05 in multivariable logistic regressions were taken as the potential determinants of community acquired pneumonia.
Data Quality Control
In order to assure the quality of the data, two-day training on independent and socio demographic data collection tool and one more day training on nutritional assessment tool was given to the data collectors. Pre-test was done on five percent of a sample at Hawassa university hospital to ensure the validity, reliability and consistency of the tool. After collecting the pretest data, each individual response was checked for any potential problem related to the data collection tool such as difficult question which discomforts the respondents in any way and difficult to understand or unclear questions etc... and corrective measures were taken. In addition, regular follow up and supervision were made by supervisors. The data collection processes were closely checked for consistency and completeness.
Result
Socio-Economic and Demographic Characteristics of the Respondent
A total of 428 (143 cases and 285 control) children aged 2-59 months and care givers /guardians were included in this study with the response rate of 100 % and 96.15 % for cases and controls respectively. Of these enrolled 86 (60.1%) cases and 174 (63.5 %) controls were permanent rural residents. The median (IQR) age of the child was 20 (27) months and 9 (17) months for cases and controls respectively. Male children accounted for 78 (54.50 %) and 141 (51.50%) for cases and control respectively. The mean (SD) ages of the mothers were 26.44 (7.41) years and 26.84 (6.76) years for cases and controls respectively. Regarding, religious status, 47 (32.9%) of case and 98 (35.8%) of control were protestant. In terms of educational status, more than half 83 (61.5%) and 103 (50.7%) of the mothers did not attend formal education for cases and control respectively. Husbands who did attend formal education were 101 (70.6%) and 119 (69.7%) for cases and control respectively (Table 3). Regarding occupational status of the mothers, 86 (60.1%) and 175 (63.9%) were housewives for cases and controls respectively. Regarding occupational status of husbands,28 (19.6%) and 45 (16.4%) were civil servants for cases and controls respectively. In terms of family size,104 (72.70 %) of cases and 118 (43.10%) of control children live in the family with more than 4 members and only 16 (3.8%) of cases and 38 (8.4 %) of control children live in the household with the number of under-five children greater than two (Table 3).
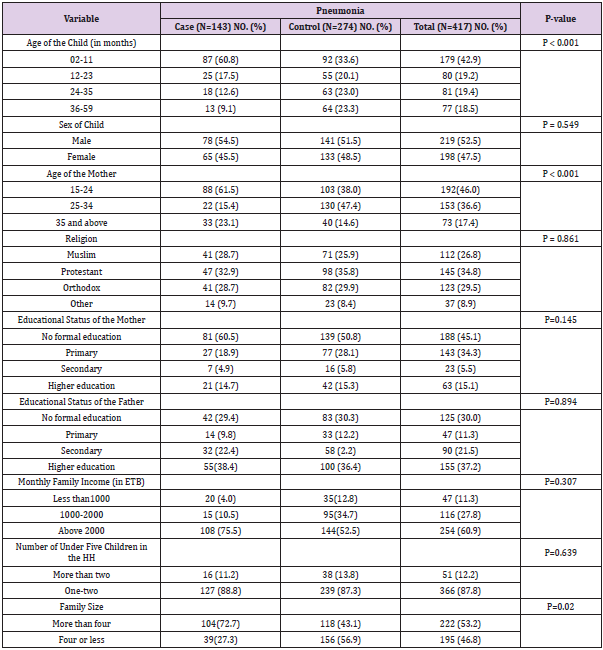
Table 3: Scio-economic and demographic characteristics of 2-59 months age children who attended health facility in Hossana town, SNNPR, Ethiopia, 2019.
Child Health and Nutrition related Characteristics of the Respondents
Regarding nutritional status of the children, 52 (36.4 %) of cases and 177 (64.6 %) of control were breastfed for more than one year. Majority of cases, 120 (83.9%) and control 257 (93.8%) were exclusively breastfed. Fifty-four (37.8%) of cases and 105 (38.3%) of control children started complimentary feeding at 6 months. Only 8 (5.6 %) of cases and 20 (7.3 %) of control were wasted. Twenty-nine (20.3%) of cases and 32 (11.7%) of control were underweight. Eighty-seven (60.8%) of cases and 89 (32.5%) of control were stunted (Table 4). More than two in ten (21.7%) of cases and 68 (24.8%) of controls had a history of RTI. Over one fourth (25.9%) of cases and 26 (9.5%) of control had a history of diarrhea. Sixty-seven (46.9%) of cases and 92 (33.6 %) of control had a history of parental RTI (Table 4).
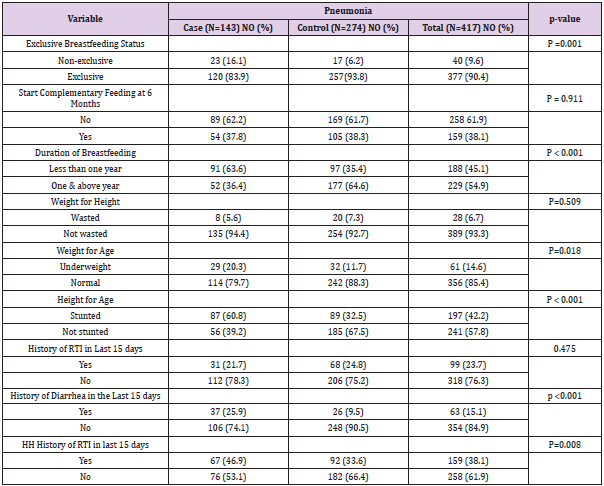
Table 4: Nutrition and health related characteristics of 2-59 months age children who attended health facility in Hossaena town, SNNPR, Ethiopia, 2019.
Vaccination Status of Children
Concerning the vaccination status of the children, only 6 (4.2%) of cases and 12 (4.4%) of control children were not vaccinated at all and the rest were vaccinated. More than half 91 (63.6 %) of cases and 179 (65.3%) of control children were fully vaccinated and the rest were vaccinated up to their age (Figure 2).
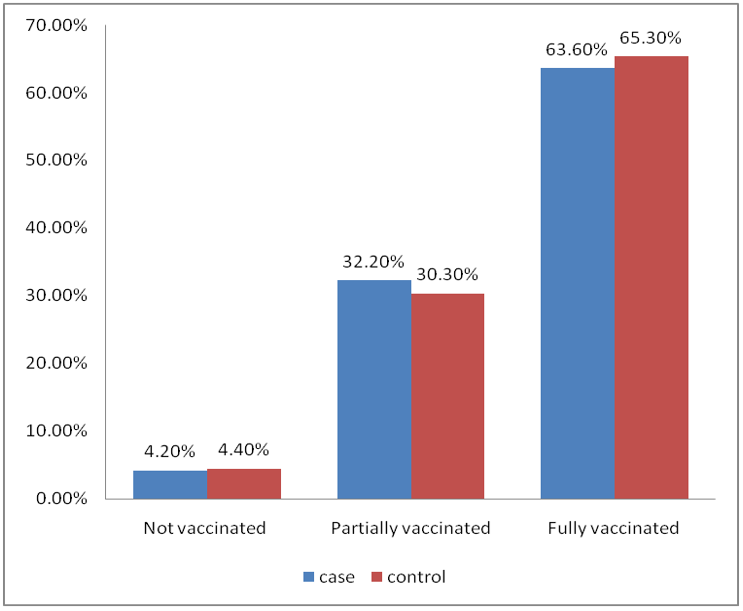
Figure 2: Vaccination status of 2-59 months age children who attended health facilities in Hossana town, SNNPR, Ethiopia, 2019.
Environmental Characteristics of the Respondents
Regarding environmental air condition, more than half of the respondents 80 (55.9 %) cases and 169 (61.7%) controls use wood as source of cooking fuel. More than one in five (22.4%) of cases and 130 (47.4%) of control cook their food in separate kitchen but around 24 (75%) and 99 (76.2%) of the kitchen do not have windows at all for cases and controls respectively. More than half 83 (58 %) of cases and 189 (69%) of controls children stayed outside the kitchen or cooking room. Over one in five (21%) of cases and 22 (8%) of control respondents reported that there are household member with cigarette smoking practice (Table 5).
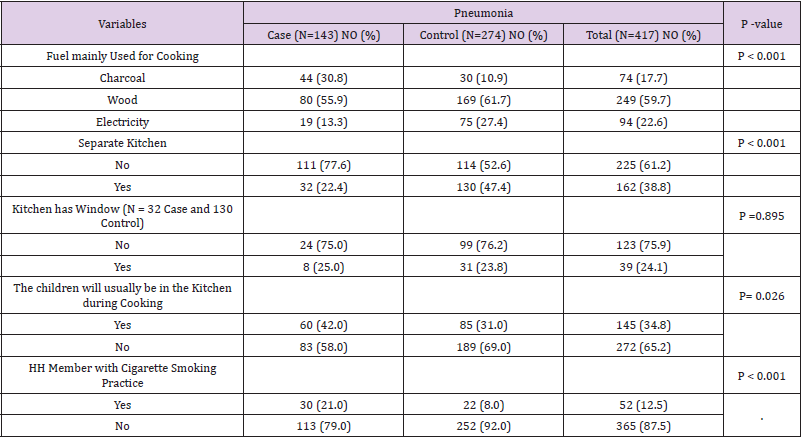
Table 5: Environmental characteristics of children age from 2-59 month who attended health facility in Hossaena town, SNNPR, Ethiopia, 2019.
Factors Associated with Community Acquired Pneumonia
Socio-Demographic and Nutrition Related Factors Associated with Community Acquired Pneumonia: In the bivariable logistic regression analysis, children who were in the age group of 2-11 months were 4.6 times (OR =4.656, 95% CI= 2.39, 9.04) and those in the age group of 12-23 months were 2.2 times (OR=2.24, 95% CI=1.04, 4.789) more likely to develop pneumonia as compared to children at age category of 34-59 months. A child born from a mother whose age is less than 25 year was 2.6 times (OR=2.66, 95% CI=1.75, 4.02) more likely to develop pneumonia compared to a child born from a mother whose age is 25 years and above. Children living in the family with more than 4 members were 2 times (OR=1.98, 95% CI=2.09, 4.86) more likely to develop pneumonia as compared to children living in the family with 4 and less members (Table 6). Children who fed breast milk for less than one year were 3.2 times (OR=3.19, 95% CI=2.1, 4.9) more likely to develop pneumonia when compared to children who fed breast milk for more than one year. Children who were not exclusively breast fed were 2.9 times (OR=2.89, 95% CI=1.49, 5.62) more likely to develop pneumonia as compared to children who were on exclusive breast feeding. Underweight children had 2 times (OR=1.92, 95% CI=1.11, 3.33) and stunted children had 3 times (OR=3.23 95% CI=2.12, 4.91) more likely to develop pneumonia than normal children (Table 6).
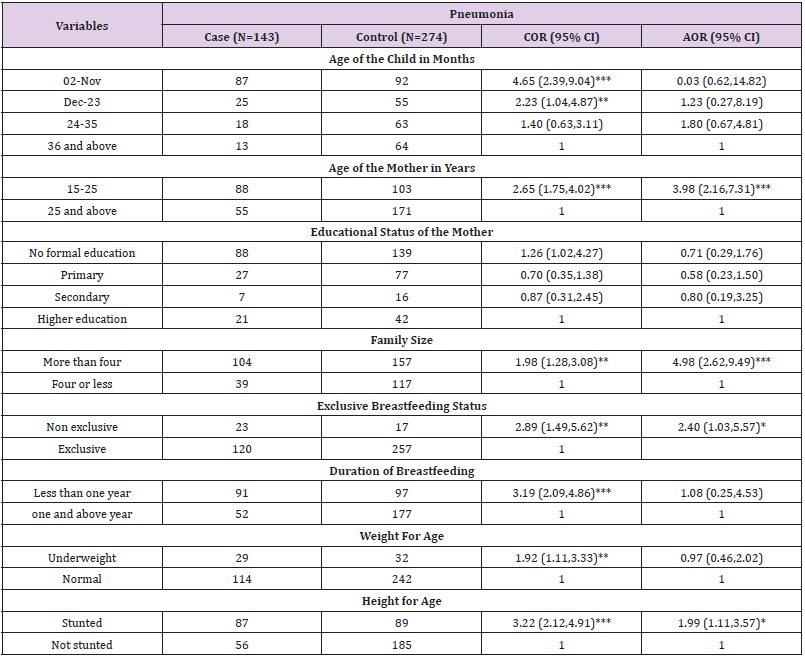
Table 6: Socio-demographic and nutritional factors associated with pneumonia using bi-variable and multi-variable logistic regression of 2–59-month children attended health facility in Hossaena town, SNNPR, Ethiopia 2019.
Note: *Significant at p-value < 0.05, **Significant at p-value between 0.01 and 0.001, ***Significant at p-value < 0.001.
Hosmer and lemeshow’s goodness of model test was found to be p – value of 0.313 which indicates the goodness of the model to predict the outcome
Environmental Health-Related Factors Associated with Pneumonia: In the bi-variable logistic regression analysis, children from families who use charcoal as a source of cooking fuel were 5.8 times (OR=5.78, 95% CI=2.91, 11.48) more likely to develop pneumonia as compared to children from the families who use electricity. Children from families who lack a separate kitchen for cooking/cook in the main house were 3 times (OR=3.13 95% CI=1.97, 4.95) more likely to develop pneumonia as compared to children from families who use a separate kitchen for cooking. Children who stayed on cooking room or on the mothers’ back while they are cooking were 1.6 times (OR=1.607, 95% CI=1.05,2.44) more likely to develop pneumonia as compared to children who stayed outside the cooking room. Children who were living with the family member with cigarette smoking practice were 3 times (OR=3.04, 95% CI=1.68, 5.504) more likely to develop pneumonia as compared to children from non-smoking parents (Table 7). Children who had history of diarrhea in the past two weeks were 3 times (OR=3.32, 95% CI=1.92, 5.77) more likely to develop community acquired pneumonia than children who have no history of diarrhea. Children from families with a history of RTI in the past 2 weeks prior to data collection were 1.7 times (OR=1.74, 95%CI=1.15, 2.63) more likely to develop pneumonia as compared to their counterparts (Table 7).
Factors Independently Associated with Community Acquired Pneumonia: After adjusting for potential confounding factors, a child born from a mother whose age is less than 25 years was 4 times (AOR=3.98, 95% CI=2.16, 7.31) more likely to develop pneumonia as compared to a child born from a mother whose age is 25 and above years. The occurrence of CAP in children living in the family with more than 4 members were 5 times (AOR=4.89, 95% CI=2.6, 9.4) higher than children who live with 4 and less family members (Table 6). The odds of having pneumonia were 2.4 times (AOR=2.4 95% CI=1.03, 5.57) more likely among children who were not exclusively breastfed as compared to children who were on exclusive breast feeding. The odds of having pneumonia are two times (AOR=2.02 95% CI=1.14, 3.61) more likely among stunted children than normal children (Table 6). Children who had history of diarrhea in the last 15 days preceding the data collection were 2.4 times (AOR=2.37 95% CI=1.13, 4.98) more likely to develop CAP than children with no history of diarrhea in the same time period (Table 7). Children from households which used charcoal as a source of cooking fuel were 6.8 times (AOR=6.89, 95% CI=2.77, 17.12) more likely to develop pneumonia as compared to children from households which use electricity. Children from family who lack separate kitchen for cooking/cook in the main house had double risk of getting CAP than children from family who use separate kitchen for cooking (AOR=2.20,95% CI=1.23, 3.91). Children who were living with the family member with cigarette smoking practice were 3.8 times (AOR=3.79, 95% CI=1.82, 7.91) more likely to develop pneumonia as compared to children from non-smoking parents (Table 7).
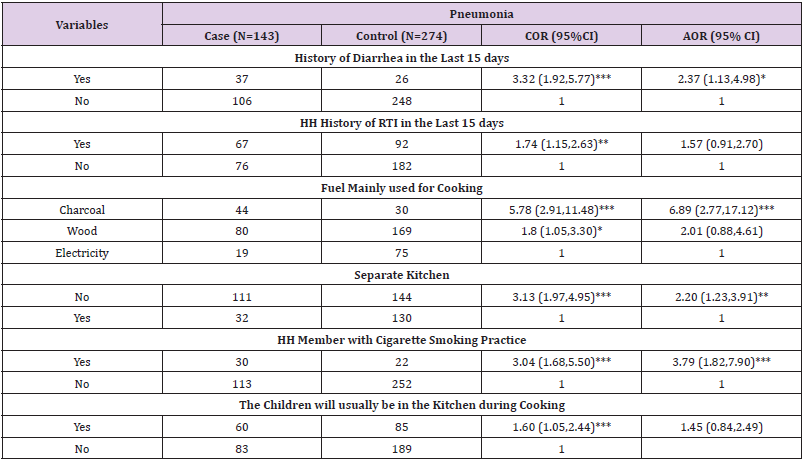
Table 7: Environmental and health related factor associated with pneumonia using bi-variable and multi-variable logistic regression of 2–59-month children attended health facility in Hossana town, SNNPR, Ethiopia 2019.
Note: *Significant at p-value < 0.05, ** Significant at p-value between 0.01 and 0.001, ***Significant at p-value < 0.001.
Hosmer and lemeshow’s goodness of model test was found to be p – value of 0.313 which indicates the goodness of the model to predict the outcome.
Discussion
Pneumonia in under-five year age children is the leading cause of morbidity and mortality in Ethiopia and other developing countries. Identifying modifiable risk factors for pneumonia could be important for proper management and prevention strategy of CAP. The result of this study identified maternal age less than 25 years as a risk factor for CAP. There were similar studies conducted in different countries which reported young maternal age as risk factor for under-five children pneumonia. For example, a casecontrol study conducted in Brazilian metropolitan area and other research report of Southeast Asian countries reported young maternal age as the risk factors for developing under-five CAP [33,34]. However, a case-control study conducted in urban area of Oromia region and across sectional study conducted in Este town and the surrounding rural kebeles, Northwest Ethiopia reported absence of association between maternal age and occurrence of CAP in under-five children [30,35].
The possible reason for this contrasting finding might be due to the different maternal age classification that the studies used based on their situations. The possible explanation for the current finding might be poor experience of younger mothers on child care and feeding. Additionally, there is higher risk of unintended and unwanted pregnancy in young mothers [36] which may lead to poor child care which might be a risk factor for occurrence of community acquired pneumonia in under-five children. In this study large family size was also identified as risk factor of CAP. This finding is in line with similar study conducted in southwest Ethiopia which identified significant association between family size and community acquired pneumonia in under-five children [37]. A cross sectional study conducted in the North West Ethiopia also showed significant association between family size and community acquired pneumonia in under-five children [35]. But another study conducted in northwest Ethiopia reported no association between family size and CAP [38]. This difference in finding could be due difference in study time which might have caused change in risk factors over time. The possible explanation could be that large family size usually connected with crowding at home which increase the transmission of respiratory tract infection through air droplet.
In this study, non-exclusive breast feeding showed significant association with occurrence of CAP. This finding is in line with a systematic review on the benefit of exclusive breast feeding that showed there were a 23 percent reduction in the occurrence of pneumonia among exclusively breastfed children [39]. A Casecontrol study conducted in North Achefer District; Northwest Ethiopia also showed that exclusive breast feeding reduced the occurrence of community acquired pneumonia by 83 percent among under-five children [38]. This difference in figures may be because the former is global study with average percent and the latter is done in a country with one the highest under five CAP burden. The possible explanation for this association could be the fact that breast feeding in early age protect infant’s (provide passive protection) against infection and has protective factor for reducing risk of respiratory illness including pneumonia. Stunting was also identified as the risk factor for pneumonia in this study. The finding is consistent with study done in Bangladesh which showed the incidence of community acquired pneumonia is significantly higher among stunted children [40]. A cross sectional study conducted in Este town and the surrounding rural kebeles, Northwest Ethiopia showed significant association between stunting and community acquired pneumonia [35].
The possible explanation for this association could be that stunting indicates long term malnutritional of the children, which weakens child’s natural body defiance mechanism and the child becomes susceptible for the disease-causing agent. Children who had history of diarrhea in the last 15 days preceding the data collection were 2.4 times more likely to develop CAP. This finding is in line with the studies conducted in different parts of the world. For instance, a study conducted in Tigray region, Ethiopia, the occurrence of community acquired pneumonia was increased among children who have history of diarrhea [41]. A Case-control study conducted in urban area of Oromia and Amhara regions, Ethiopia, also showed significant association between diarrhea and community acquired pneumonia in under-five children; children who had history of diarrhea in the past two weeks were 3 times more likely to develop community acquired pneumonia than children who have no history of diarrhea [30]. Children who have concomitant illness like diarrhea which may compromise their nutritional status, have a lowered immunity and making them more susceptible to infectious agent including pneumonia. From the variables related with indoor and environmental air pollution, use of charcoals as a source of cooking fuel shown statistically significant association with community acquired pneumonia in under-five children. This finding is consistent with study conducted in Este town, North-west Ethiopia which showed significant association between charcoal use and community acquired pneumonia in under-five children [35]. This might be due to higher environmental/indoor air pollution from charcoal/wood use; air pollutants may adversely affect host defense mechanism of the air way against pathogens.
Lack of separate kitchen for and cooking in the main house were also other factors identified as a risk factor for community acquired pneumonia in under-five age children. This finding is consistent with a case-control study conducted in Ndola, Zambia, which showed significant association between not having separate room for cooking and occurrence of acute respiratory tract infection in under-five children [42]. A cross sectional study conducted in Kenya also showed significant association between cooking near bed and acute respiratory tract infection in underfive children [43]. Similar result is also reported at a cross sectional study conducted in Wondogenet district in Sidama zone, Ethiopia, which showed that absence of separate kitchen was 6.83 times higher risk for the acquirement of community acquired pneumonia in under-five age children [29]. In these cases, risk of household air pollution is high, which contributes to pulmonary inflammation and tissue damage that favors the growth of ethologic agent and increase susceptibility of children to acquire pneumonia [3]. Finally, cigarette smoking was identified as risk factor for CAP; children who were living with the family member with cigarette smoking practice were 3.7 times more likely to develop pneumonia as compared to children from non-smoking parents. The result is supported by a prospective cohort and case-control study conducted in England and Gambia respectively showed significant association between household cigarette smoking and community acquired pneumonia in under-five children [44,45]. A case-control study conducted in southwest Ethiopia also showed significant association between household cigarette smoking and occurrence of community acquired pneumonia in under-five children, identified household cigarette smoking as independent risk factor for the occurrence of community acquired pneumonia in under-five children [37]. But a case-control study conducted in Brazilian metropolitan area and a cross sectional study conducted in northwest Ethiopia reported that there were no association between parental cigarette smoking and the occurrence of community acquired pneumonia in underfive children [34,35]. This difference in the findings may be due to the study’s failure to indicate whether the smoking is indoor or outdoor. The possible explanation for the current finding could be that smoking contributes to the particulate load in indoor air and inhaling particles which limit the action of mucus and leading to cough in children. Further it causes lung tissue damage which leads to accumulation of fluid and favors the growth of disease-causing agent [46-51].
Conclusion
The risk factors of community acquired pneumonia were maternal age less than 25 years, family size greater than four, nonexclusive breast feeding, stunting, history of diarrhea in the last 15 days, wood and charcoal used as a source of cooking fuel, lack of separate kitchen and parental smoking.
Strength and Limitation of the Study
The strength of the study was being case control study design and its limitation was health facility controls were used; community/neighborhood control would offer better comparison and given interviewers a chance to observe environmental and housing condition and used to limit social desirability bias; and there is age discrepancy between case and control which in turn made the comparison difficult.
Declaration
Data Sharing Statement
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request by using this email yeshaayele@yahoo.com.
Ethical Approval and Consent to Participate
In order to carry out this study, ethical clearance was obtained from Hawassa University institutional review board. Written consent form was also taken from the guardian of the child after informing the objective of the study. All methods were performed in accordance with Ethiopian national research ethics guideline for those researches involving human being.
Author Contributions
Adis Endale, Taye Gari, Yusuf Haji, Yeshanew Ayele and Taye Wudneh were contributed in writing, revising, editing, analysis and interpretation and the Adis Endale and Yeshanew Ayele also contributed in manuscript preparation.
Funding
No fund for this study.
Acknowledgment
We would like to thank study participants, data collectors, supervisors and Hawassa and Wachamo University.
Disclosure
All authors don’t have any conflict of interest.
References
- Kliegman R, Stanton B, Geme J (2008) Nelson Textbook of pediatrics (19th)., In: Kliegman R, Stanton B, Geme J (Eds.)., Elsevier Saunders, Philadelphia, pp. 1142-1151.
- Rudan I, Boschi Pinto C, Biloglav Z, Kim Mulholland, Harry Campbell (2008) Epidemiology and etiology of childhood pneumonia. Bull World Health Organ 86(5): 408-419.
- Liu L, Oza S, Dan H, Yue C, Jamie P, et al. (2016) Global, regional, and national causes of under-5 mortality in 2000–15: an updated systematic analysis with implications for the Sustainable Development Goals. Lancet 388(10063): 3027-3035.
- Wardlaw T, Salama P, Johansson W (2006) Pneumonia: The leading killer of children. Lancet 368(9541): 1048-1052.
- Walker L, Rudan I, Liu L, Harish Nair, Evropi Theodoratou (2013) Global burden of childhood pneumonia and diarrhea. Lancet 381(9875): 1405-1416.
- (2014) UNICEF. Country estimates of child mortality, causes of under-five deaths and coverage indicators in committing to child survival: A promise renewed progress report.
- Deribew A, Tessema F, Girma B (2007) Determinants of under-five mortality in Gilgel Gibe Field Research Center, Southwest Ethiopia. Ethiop J Health Dev 21(2): 19-21.
- Ashworth A, Bickler S, Deen J (2013) Pocket book for hospital cares for children: Guidelines for the management of common illness with limited resources. Amsterdam: KIT press 2013: 68-83.
- Leowski J (1986) Mortality from acute respiratory infections in children under 5 years of age: Global estimates. World Health Statistics Quarterly 39(2): 138-144.
- (2008) UNICEF. Chart booklet: Integrated Management of Childhood Illness (IMCI). Geneva World Health Organization/The United Nation Children’s Fund.
- Dempsey J, McArdle F, Morris J, Lloyd Evans N, Baldeh I (1996) A Study of Risk Factors for Pneumococcal Disease among Children in a Rural Area of West Africa. Int J Epidemiol 25(4): 885-893.
- (2002) WHO. The Multi-Country Evaluation of IMCI Effectiveness, Cost and Impact (MCE) – Progress Report. Geneva: World Health Organization.
- Schellenberg J (2003) Inequalities among the very poor. Health care for children in rural southern Tanzania. Lancet 361(9357): 561-566.
- Schumacher R, Eric Swedberg, Mamadou Oury Diallo, Damou Rahim Keita, Henry Kalter, et al. (2002) Mortality Study in Guinea: Investigating the causes of death in children under 5. Virginia: Save the Children and the Basic Support for Institutionalizing Child Survival (BASICS II) Project.
- (2014) UNICEF. Integrated Management of Childhood Illness (IMCI) (revised) Geneva, World Health Organization/The United Nation Children’s Fund.
- (2013) WHO. Pocket book of hospital care for children: Guidelines for the management of common illnesses. Geneva: World Health Organization.
- (2012) WHO. Recommendations for management of common childhood conditions, Evidence for technical update of pocket book recommendations. Geneva: World Health Organization.
- Wardlaw T, You D, Newby H, Anthony D, Chopra M (2013) Child survival: a message of hope but a call for renewed commitment. UNICEF report 10: 64.
- Memirie T, Metaferia S, Norheim F (2017) Household expenditures on pneumonia and diarrhea treatment in Ethiopia. a facility-based study. BMJ Global Health 2(1): 000166.
- Azad K (2009) Risk factors for acute respiratory infections (ARI) among children under five years in Bangladesh. Journal of Scientific Research 1(1): 72-81.
- Dadi F, Kebed Y, Birhanu (2014) Determinants of Pneumonia in Children Aged Two Months to Five Years in Urban Areas of Oromia Zone, Amhara Region, Ethiopia. Open Access Library Journal 1(8): 01-10.
- Ali M, Asfaw T, Beyne H, Byass P, Shisay M, et al. (2001) A Community Based Study of Childhood Morbidity in Tigray, Northern Ethiopia. Ethiopian Journal of Health Development 15: 165-172.
- Teshome A (2017) Prevalence of pneumonia and factors associated among children 2-59 months old in Wondo Genet district, Sidama zone, SNNPR, Ethiopia. CurrPediatr Res 21(1): 19-25.
- Fekadu A, Terefe W, Alemie A (2014) Prevalence of pneumonia among under-five children in Este Town andthe surrounding rural Kebeles, Northwest Ethiopia: A community based cross sectional study. Journal of Public Health 2(3):150-155.
- Geleta D, Tessema F, Ewnetu H (2016) Determinants of Community Acquired Pneumonia among Children in Kersa District, Southwest Ethiopia: Facility Based Case Control Study. J Pediatr Neonatal Care 5(2).
- Yohannes T, Laelago T, Ayele M, Tamrat T (2017) Mortality and morbidity trends and predictors of mortality in under-five children with severe acute malnutrition in Hadiya zone, South Ethiopia: a four-year retrospective review of hospital-based records (2012–2015). BMC nutrition J 3(18).
- (2016) WHO. Towards a Grand Convergence for Child Survival and Health, A strategic review of options for the future building on lessons learnt from IMNCI. WHO Switzerland: WHO Geneva.
- Efrem T, Dedefo T, Ismael A, Hibret A, Tesfaye B (2014) Quality and use of imnci services at health center under-five Clinics after introduction of integrated community-based case Management (iccm) in three regions of ethiopia. Ethiop Med J 3: 91-98.
- Liu L, Oza S, Hogan D (2014) Global, regional and national causes of child mortality in 2000-13, with projections to inform post-2015 priorities: an updated systematic analysis. The Lancet 385(9966): 430-440.
- Admasu K (2014) Integrated community case management of sick children in ethiopia. Ethiop Med J 52.
- (2011) Central statistics authority Ethiopia demographic and health survey. Addis Ababa, Ethiopia.
- Gordon D, Frenning S, Draper H, Kokeb M (2013) Prevalence and Burden of Diseases Presenting to a General Pediatrics Ward in Gondar, Ethiopia. Journal of Tropical Pediatrics 59(5): 350-357.
- Onyango D, Kikuv G, Amukoye E, Omolo J (2012) Risk factors of severe pneumonia among children aged 2-59 months in western Kenya: a case control study. Pan African Medical Journal 13: 45.
- Ahmed A (2011) Retrospective analyses of pattern and outcomes severe pneumonia in children at Jimma University Specialized Hospital,Jimma. JimmaUniversity 5: 26-33.
- White F (2002) A comparison of ‘cough and cold’ and pneumonia: risk factors for pneumonia in children under 5 years revisited. International Journal of Infectious Diseases 6(4): 295-301.
- Tessema F, Ewnetu H (2016) Determinants of Community Acquired Pneumonia among Children in Kersa District, Southwest Ethiopia: Facility Based Case Control Study. J Pediatr Neonatal Care 5(2): 00179.
- Firaol B, Javed A, Abhay K, Tabarak M (2017) Factors associated with outcomes of severe pneumonia in children aged 2 months to 59 months at jimma university specialized hospital, southwest Ethiopia. jimma university 21(3): 447-454.
- Cutts F, Zaman S, Enwere G, Jaffar S, Levine O, et al. (2005) Efficacy of Nine-Valent Pneumococcal Conjugate Vaccine against Pneumonia and Invasive Pneumococcal Disease in the Gambia: Randomized,Double-Blind, Placebo-Controlled Trial. Lancet 365(9465): 1139-1146.
- Portela M, Sant’anna C, Campos J (2005) Pneumonia emcrianças e adolescents indígenas internados em Brasília- DF: estudo de casos. Pulmão RJ 14(4): 283-288.
- Orellana J, Basta P, Santos R (2007) Morbidade hospitalar em crianças indígenas Suruí menores de dezanos, Rondônia, Brasi. Rev Bras Saúde Mater Infant 7(3): 281-287.
- Gedefaw M, Berhe R (2001) Determinates of Childhood Pneumonia and Diarrhea with Special Emphasis to Exclusive Breastfeeding in North Achefer District, Northwest Ethiopia: Case Control Study. Open Journal of Epidemiology 5(2): 107-112.
- Bernardo H, Cesar V (2013) Short-term effects of breastfeeding: a systematic review on the benefits of breastfeeding on diarrhoea and pneumonia mortality. WHO Libr Cat Data 1(3): 49.
- Puchalski R, Howie S, Arenovich T, Cheung Y Weber M, Moore S (2009) Long-Term Morbidity from Severe Pneumonia in Early Childhood in the Gambia West Africa. A Follow-Up Study. International Journal of Tuberculosis and Lung Disease 13(4): 527-532.
- Teepe J, Grigoryan L, Verheij T (2010) Determinants of community acquired pneumonia in children and young adults in primary care. EurRespir Journal 35(5): 1113-1117.
- Maliha N, Zafar F, Arif A (2011) Effect of Behavioral Risk Factors on Development of Pneumonia among Children Under-5 Years of Age: A Case-Control Study. Malaysian Journal of Paediatrics and Child Health 1(7): 1-17.
- Victora C, Fuchs S, Flores J, Fonseca W (1994) Kirkwood B. Risk factor for pneumonia among children in Brazilian Metropolitant area. Open J of Pediatrics 39(6): 977-985.
- Banda B (2016) Risk factors associated with acute respiratory infections among under-five children admitted to Arthur’s Children Hospital, Ndola, Zambia. Asian Pac J Health Sci 3(3): 153-159.
- Sikolia N, Mwololo K, Cherop H (2002) The Prevalence of acute respiratory infections and the associated risk factors: A study of children under five years of age in KiberaLindi Village, Nairobi, Kenya. J Natl Inst Public Health 51(1): 67-72.
- Strachan P, Cook G (1997) Health effects of passive smoking. Parental smoking and lower respiratory illness in infancy and early childhood 52(10): 905-914.
- Turner C, Turner P, Carrara V, Burgoine K, Tha Ler Htoo (2013) High Rates of Pneumonia in Children under Two Years of Age in a South East Asian East Asian Refugee Population. PloS One 8(1).
- Belayneh H, Abebe Gm, Tizta T (2012) Unwanted Pregnancy and Associated Factors among Pregnant Married Women in Hosanna Town, Southern Ethiopia. PLoS One open, Open access journal 7(6): e39074.
