 Research Article
Research ArticleABSTRACT
Background: The International Health Regulations (IHR 2005) is coordinated by the WHO as an instrument aimed to capable countries to respond to public health events it firstly adopted in Gaza Strip (GS) in 2009.
Aim: To assess the existing IHRs` core capacities against public health events in Palestine.
Methods: A combination of qualitative research methodologies was conducted; purposive sampling was used to conduct in-depth interviews with forty-three key informants; WHO’s Joint External Evaluation tool was used to assess the IHR core capacities; the study conducted in GS governorates.
Results: The results revealed that 44 % have no knowledge about the IHR and 84 % of them did not know who is the IHR`s focal person of in GS. There was better capacity in the detection core function whereas low capacity in response and prevention core functions.
Conclusion: IHR`s ‘2005” is poorly demonstrated in GS with an obvious lack of national coordination; it`s essential and crucial to the Palestinian health care system to strengthen and support the implementation of IHR`s “2005” in order to respond to public health emergencies and adhere with WHO`s recommendations.
Keywords: Palestine; Health System Analysis; International Health Regulations (IHR 2005); Joint External Evaluation; Crises
Abbreviations: JEE: Joint External Evaluation; MoH: Ministry of Health; GS: Gaza Strip; IDIs: In-Depth Interviews; LNGO: Local Non-Governmental Organization; QDA: Qualitative Data Analysis
Introduction
Joint External Evaluation (JEE) tool is a voluntary, collaborative, multisectoral process to comprehensively assess country capacity to prevent, detect and rapidly respond to public health risks in the framework of the International Health Regulations. The International Health Regulations (IHR 2005) is a legal instrument aiming to improve countries’ ability to protect and respond to international health threats, including epidemics, it covers measures for preventing the transnational spread of infectious diseases [1- 3]. The IHR 2005 was first adopted in 1969. IHR 2005 was thus adopted by the World Health Assembly in May 2005 and came into force in 2007 for 194 countries [4,5]. Developing countries, are expected to suffer from inability to implement the IHR 2005 [6]. In 2015, an elucidated gaps including a limited capacity in detecting infectious pathogens were identified after qualitative assessment to evaluate the IHR capacities in Palestine [7]. In December 2019, China reported COVID-19 cases, then in Jan 2020, WHO declared COVID-19 as greatest public health emergency [8-10]. Palestine is highly vulnerable to a variety of natural and human-made hazards; Disaster risk reduction, emergency preparedness and response are therefore of high priority for the Ministry of Health (MoH) and its partners [11].
Gaza Strip (GS) is a 365 km2 piece of land, inhabited by more than 2 million Palestinians; This open-air enclave has been under siege for the past 14 years, it was exposed in the last years to several wars which has left the health system jeopardized by failing equipment and limited resources and essential drugs [12]. This situation was worsened by COVID-19 pandemic [13]. The last war in May 9, 2021, the Israeli Government launched a military offensive against GS. The Palestinian Ministry of Health (MoH) has reported at least 253 Palestinians killed and about 1948 Palestinians wounded [14]. More than 120,000 citizens left their homes in search of safety [15]. 89 violations against the health sector, included injuries of health workers and complete or partial damage to health facilities [16,17]. In addition to lack of electricity resources to became available in 3 to 4 hours per day [18]. The Palestinian MoH response to Covid-19 outbreak and other public health emergencies is undermined in GS due to lack of proper regulations and strategies, which are crucial to public health security.
General objective
To assess the existing IHRs` core capacities against public health events in Palestine.
Methods
A combination of qualitative research methodologies was conducted; purposive sampling was used to conduct In-Depth Interviews (IDIs) with forty-three key informants; The study was conducted throughout GS, Palestine. The study included healthcare sectors “governmental sector, United Nations Relieve and works Agency sector (UNRWA), medical military services, Local Non- Governmental Organizations (LNGOs), Academics and health consultants. The researcher used modified and simulated Joint External Evaluation (JEE), IHR (2005) tool, [19] published by WHO to assess country capacity to prevent, detect, and response to public health threats. Four data analysis steps were followed, in order to gain insight into the key informants’ perceptions of the implementation of the IHR (2005) in GS. First, the interpretation of the data by reading each transcript and underlining statements. Second, all underlined statements were coded across each interview undergoing inductive analysis. Third, all codes were grouped into two themes: positive perceptions and negative perceptions. Four, all statements in both themes were read and reviewed to reflect the overarching key health informant’s perceptions about the implementation of the IHR (2005).
The qualitative data were analyzed [20] as follow:
• Qualitative questions were analyzed by using inductive approach in the Qualitative Data Analysis (QDA),
• Manual thematic content analysis of transcripts and interview notes were applied,
• Data were taped, recorded and transcribed,
• The interviewers reported notes of key points arising and verbatim quotes,
• Coding scheme and coding the data by relevant labels and categorization were created.
The qualitative data analysis was done by using the key informants’ quotes to develop scoring for the indicators of IHR core capacities based on World Health Organization’s JEE tool which developed to evaluate the IHR core capacities globally. The JEE tool number-scoring for the core capacities indicators is designed in the form of a five-number scale [1-5].
Results
In GS, most indicators of the IHR core capacities classified under the three core functions “prevention, detection and response” were scored from 1 “no capacity” to 5 (sustainable capacity), whereas it was 3 “developed capacity” in average. One indicator “vaccine coverage” out of forty-two indicators was classified as sustainable capacity, twelve indicators (28.5%) were classified as demonstrated capacity, 45 % (19/42 indicators) were listed under category of developed capacity, eight indicators (19%) were classified as limited capacity and two indicators listed under no capacity classification.
Prevention
As revealed in Table 1, there are fifteen prevention indicators in this evaluation. One indicator “biosafety and biosecurity training and practices” showed no capacity, 7/15 indicators showed limited capacity such as Antimicrobial Resistance (AMR) detection and surveillance of infections caused by its pathogens, one indicator “antimicrobial stewardship activities” listed under score 3 “developed capacity”, five indicator showed demonstrated capacity score number “4” and one indicator “ vaccine coverage “Measles” as part of national program” showed sustainable capacity.
Detection
Detection core function included thirteen indicators. There were no indicators showed sustainable capacity; demonstrated capacity, limited capacity and no capacity listed with one indicator to each one as follows laboratory quality system, indicatorand event-based surveillance systems and workforce strategy respectively, whereas ten indicators revealed developed capacity with score “3”, Table 1.
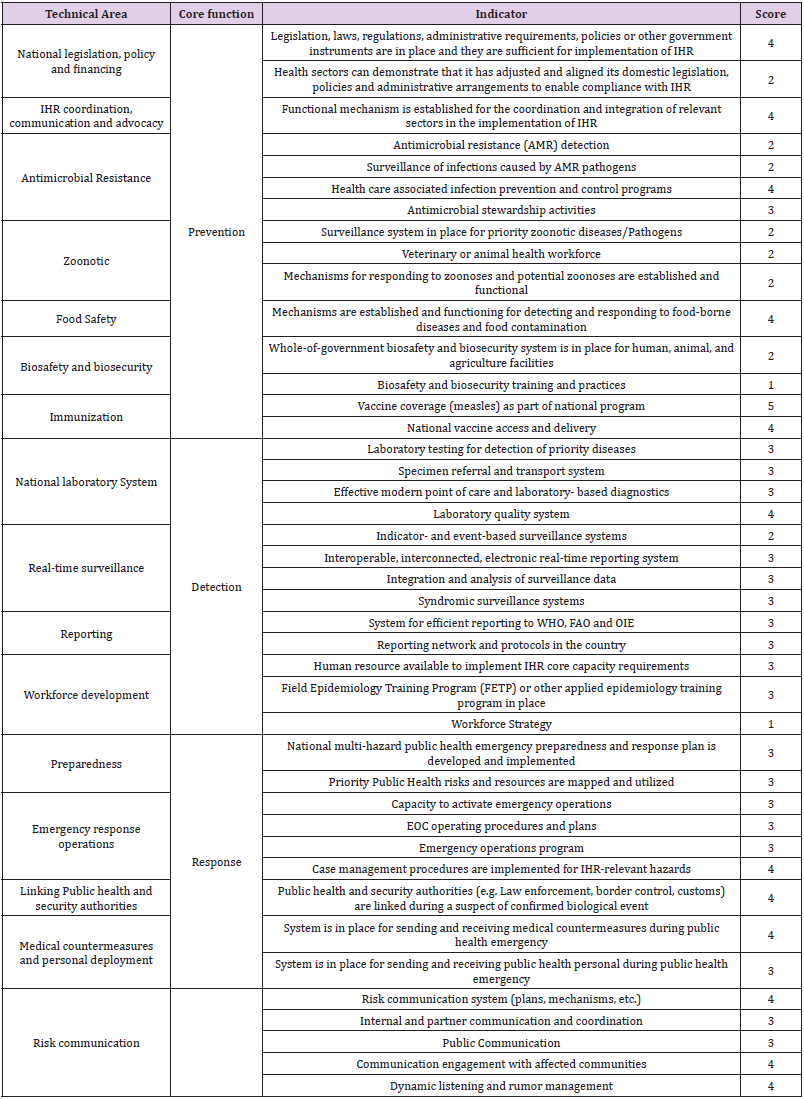
Table 1: IHR Core Capacities Scoring in GS, Palestine – 2022.
Note: Score 1; No capacity; score 2: Limited capacity; score 3: Developed capacity; score 4: Demonstrated capacity; score 5: Sustainable capacity
Response
As clarified in Table 1 the response core function considered the best one with comparison to the other core functions “prevention and detection”. Fourteen indicators were included in this category, eight indicators scored “3” showing developed capacity, 6 indicators showed demonstrated capacity with score “4”, whereas there were neither indicator to no capacity, limited capacity nor sustainable capacity.
Discussion and Conclusion
The findings of this evaluation indicating that IHR`s ‘2005” adopted in GS in 2009 and it`s poorly demonstrated in GS with better capacity in the detection core function and low capacity in response and prevention core functions. In spite of fragile health care system due to conflict, ongoing blockade, resources shortages and recurrent public health emergencies the implementation of the IHR`s 2005 is corrupted and lack or no national coordination in place, mainly because of the political division in Palestine. With focusing on the results as shown in Table 1 indicating that GS has low capacity in response and prevention core functions whereas better capacity in the detection core function. As expressed by the focal person in GS “national coordination related to IHR 2005 is corrupted”; the political division in Palestine has bad impact to support the implementation of the IHR`s 2005 core capacities. Most of key informants (38/43) revealed that there is functional mechanism for the coordination and integration between the working health sectors in GS in case of emergencies and the epidemiology and crises committee is formulating.
Lack of financial resources, lack of vaccines, rumors and siege are the main obstacles in the immunization program (33/43). As thirty-three key informants said “community encouragement and education, reviewing of immunization registers, defaulter`s follow up and monitoring of birth numbers” are essential to monitor and maintain high immunization coverage. Availability of electricity all times, supervisory visits and Vaccine Vial Monitors (VVM) are crucial to maintain cold chain (30/43); electricity was available in the GS on a rotating basis for 8 hours, so the health care system provided most of the health care facilities with solar system and generators to ensure available electricity all time [21]. To maintain and guarantee successful and sustainable immunization program the health care system must maintain vaccination`s stocks and allocating a budget for vaccinations within the budget of the MoH (38/43) In Palestine as well as GS, the immunization considers a success story and strong prevention program, as the key informants (40/43) expressed vaccination coverage scored 5 “sustainable capacity” and Bagcchi`s study revealed that the median of vaccination coverage of measles was 97 % during 2009 to 2018 [22].
Two key informants said that screening of Anti-Microbial Resistance (AMR) is conducted in the universities as a research activity but there is no national program. The basic labs are well equipped but advanced labs not well equipped (16/43). In GS, we have governmental not national laboratories’ committee and we need quality control and assurance program to monitor the laboratory activities (19/43). The Palestinian healthcare system using different meant to notify the communicable diseases such as telephone, fax, e mail, paper notification and the MoH is the responsible for the surveillance activities with partnership with other sectors working in GS (29/43). Data`s verification conducting through regular supervisory visits, reviewing records and monitoring the numbers of reported cases (9/43). Lack of feedback to health care providers notifying about the communicable disease consider big threat to sustain notification system (30/43). There is a plan to electronically transform the surveillance system including different sectors providing the health services in GS (1/43).
In GS, we have no guideline to response to emergencies but we have unified plan (14/43) in case of epidemics, emergencies and/ or new events decision makers met continuously and deciding the procedures to respond to these public health emergencies and issuing informative reports (19/43), in spite of workload during public health emergencies there is no promotion system in GS. In place we have national training program to build capacity of the health care providers especially those working in response to public health emergency (31/43).
In case of public health emergency in GS, we respond to it by implementing the emergency plan that is developed previously and training the healthcare providers how to respond with resources mapping and utilization, three times simulation training were conducted to respond to COVID-19 pandemic prior reporting of the first case in August 2020 (29/43). In GS, there is health quarantine law as mentioned in the Palestinian public health law and in response to the public health emergency, there is public health and security authorities’ linkage but not written (32/43) [23,24].
System is in place for sending and receiving medical countermeasures and public health personnel during public health emergency (31/43). Risk communication system is available in GS (33/43), also the internal and partner communication and coordination is in place (30/43); well-trained focal communication spokesman to the MoH is available, in addition to rumor`s frightening activities.
Recommendation
The researcher recommended formulation of an integrated multi-sectoral committee of the IHR`s “2005”, enhancement of national coordination and strengthening of the health system and supporting the implementation of IHR “2005”.
Author Statements
Acknowledgment
The researcher would like to acknowledge all key informants for their support and assistance, special thanks to all data collection and processing team.
Ethical approval
All required ethical approval letters to conduct the study were taken from the relevant ethical institutional committee.
Funding
This work was supported by Eastern Mediterranean Regional Office (EMRO), World Health Organization (WHO), with Grant Number AP21-00528.
Competing Interests
None.
References
- Katz R, Standley CJ (2019) Regional approaches for enhancing global health security. BMC Public Health 19.
- Aldis W (2008) Health security as a public health concept: a critical analysis. Health Policy and Planning 23(6): 369-375.
- WHO, EMRO. International Health Regulations (IHR).
- Lee J (2020) IHR 2005 in the Coronavirus Pandemic: A Need for a New Instrument to Overcome Fragmentation? The American Society of International Law 24(16).
- Frequently asked questions about the International Health Regulations (2005).
- Bakari E, Frumence G (2013) Challenges to the implementation of International Health Regulations (2005) on Preventing Infectious Diseases: experience from Julius Nyerere International Airport, Tanzania. Glob Health Action 6(10):
- (2017) The Norwegian Institute of Public Health (NIPH). Global Health Preparedness Project in Palestine.
- Novel Coronavirus (2019-nCoV) SITUATION REPORT – 1, 21 JANUARY 2020.
- Priority Diseases, Prioritizing diseases for research and development in emergency contexts.
- Perlman S (2020) Another Decade, Another Coronavirus. N Engl J Med 382(8): 760-762.
- WHO, EMRO. Country Cooperation Strategy for WHO and the Occupied Palestinian Territory 2017–2020.
- Awadallah I, Elessi K (2021) An acute-on-chronic health crisis in Gaza. The Lancet, Correspondence, On line version.
- Felesteen online. Press release from the Preventive Medicine Directorate, 25 April 2021.
- Palestinian Ministry of Health (PMoH), GS. An update of the total victims of the Israeli aggression on the Gaza Strip. 24 May 2021, 10:30 pm.
- The Ministry of Public Works and Housing. A press release issued by the Ministry of Public Works and Housing regarding the ongoing Israeli aggression on the Gaza Strip, 20 May 2021.
- MoH, Ramallah (2021) A press release issued by the Ministry of Health regarding the Israeli aggression on the Gaza Strip.
- MoH, GS (2021) A press release issued by the Ministry of Health regarding the Israeli aggression on the Gaza Strip.
- BBC News. Gaza and Israel: What is life like in the Gaza Strip? 21 May 2021.
- (2020) Academy to Innovative Human Resources (AIHR). The Interview Guide: 7 Key Elements.
- Joint external evaluation tool: International Health Regulations (2005).
- Caulfield J. How to do thematic analysis? Scribbr, 2019.
- Abu Ali K (2021) COVID-19 and the Armed Conflict on Gaza, The Palestinian Healthcare System Response. J Gynecol Women’s Health 22(2).
- Bagcchi S (2020) Measles returns to the Gaza Strip. Lancet Infect Dis 20(3): 291.
- Palestinian News and Info Agency. Public health law, 2004. Version 20.
