 Review Article
Review ArticleSUMMARY
Antiemetic drugs have been used frequently in various areas of modern medicine, however there is a tendency to underestimate their adverse effects at the neurological level or in some cases they are unknown by the doctors who prescribe this medication. Extra pyramidalism syndrome due to metoclopramide is a clinical picture that occurs in patients who use this medication as a base therapy for vomiting, nausea or gastrointestinal discomfort, although it may exist in some cases of this drug with either poor dosage or misuse for suicidal purposes, it is estimated that it occurs in 1 in 500 patients, being a fairly significant adverse effect at present, which has led to conditioning its use in different population groups such as the elderly and pediatric patients.
Keywords: Extrapyramidalism; Intoxication; Metoclopramide; Vomiting
Abbreviations: WOK: Web of Knowledge; Meto: Metoclopramide; Ach: Acetylcholine; NANC: Non-Adrenergic-Non-Cholinergic Transmitter
Introduction
Antiemetics are mainly used in different areas of medicine, in specific groups of patients, such as those at high risk of nausea and vomiting in the postoperative period [1]. Also in those undergoing chemotherapy or palliative care; population groups have been described around which their use is a controversial issue, such as the pediatric population. Because of this, in 1996, the American Academy of Pediatrics issued a consensus, which does not recommend the use of antiemetics in children with gastroenteritis and instructs health service employees to take into account their potential adverse effects at the neurological and cardiovascular level [2,3].
Historically the molecule was discovered in 1953 and is patented on April 6, 1982 by Michel Thominet, who obtained it from orthoramides, this derivative of the nucleus of procaine and very close to pronestyl and chloroprocain, as we see despite being part of this family of drugs, we find that it has completely different pharmacodynamic actions, which have to date scientists surprised by its paradoxical pharmacological actions, that is, for example it can cause both hyperkinesis and relaxation; that is, it shares a parasympatholytic effect and a morphine one, thus being a molecule of high scientific interest [4,5]. However, the mechanism of action of metoclopramide is complex, it describes the pathophysiological bases of its neurotoxic effects in different patients, thus causing extrapyramidal syndrome, which is a complex clinical syndrome that occurs mainly in the pediatric population, although it has been documented that it can occur in a certain percentage of elderly people as an adverse effect of this drug or in case of presenting an overdose of this same, despite this a significant percentage of health providers who care for children with gastroenteritis prescribe antiemetics, of which at least 10% continue with these drugs on an outpatient basis [6,7]. Due to its frequent use and the tendency to underestimate or ignore the severity of neurological adverse reactions, this article aims to review the literature on metoclopramide poisoning and other antiemetics frequently used today and its clinical approach to each particular step.
Methodology
The study design was that of a systematic review of the evidence present in the scientific literature on metoclopramide poisoning. The literature search took place between January and February 2022, delving into various bibliographic databases in order to obtain information and review previous studies on the subject exposed. The databases used were Pubmed-Medline, Web of Knowledge (WOK) and SCOPUS, in which the search strategies differed depending on the source used. The keywords and Boolean operators used were “OR intoxication “Metoclopramide” “Extrapyramidal syndrome” AND “Vomiting” described through DeCS (Descriptors in Health Sciences). To achieve a greater update on the subject, the articles published in the last 20 years were set as a temporary filter for the search.
Results
Metoclopramide and Extrapyramidalism
Extrapyramidalism caused by metoclopramide has been observed in one in 500 patients, usually women, children, and the elderly. On the other hand, in the Caucasian population, the reported data of extrapyramidalism due to metoclopramide is only 1:1500 in this population group, despite the fact that, in 5-10% of the population, it is poor metabolizer of cyp2d6 that is responsible for metabolizing the vast majority of drugs [8]. This prokinetic antiemetic of the group of orthoramides, which block serotonergic receptors 5-ht4 and dopaminergic, Derived from the nucleus of procaine, Professor Justin Besancon found that a derivative of procainamide 2-methoxyprocamide, (Figure 1) that was being studied as antiarrhythmic also showed antiemetic properties. Although its mechanism of action is more complex and in it its effects are explained (Table 1).
Figure 1: Molecular structure of metoclopramide.
Table 1: Physico-chemical information of Metoclopramide.
Note: Taken from Velázquez Basic and Clinical Pharmacology [9].
Mechanism of Action of Metoclopramide
Metoclopramide (Meto) is responsible for activating the 5-HT4 receptors of excitatory interneurons, which increases the release of acetylcholine (Ach), from the primary motor neurons of the myenteric plexus, this being its main action. However, it is possible that they also block the 5-HT3 receptors of the inhibitory interneurons responsible for relaxation by release of the nonadrenergic- non-cholinergic transmitter (NANC), which is added to the increased release of Ach, by the primary motor neuron, in addition metoclopramide also has effects on the D2 receptor blocking it, which is normally responsible for inhibiting the release of Ach by the primary motor neuron [9] (Figure 2). The best defined action is antiemetics and this is thanks to the fact that its area of action is located on the floor of the fourth ventricle, in the chemo sensitive zone, in the trigger zone, which is called an activated chemoreceptor zone molecules of a very diverse chemical nature that stimulate vomiting. The postrema is an area that has no blood-brain barrier, which allows various chemical compounds to access through it with ease [10]. Metoclopramide due to its various pharmacokinetic actions can cause paradoxical extrapyramidal symptoms such as akathisia, serotonin syndrome, tardive dyskinesia and neuroleptic malignant syndrome. Extrapyramidal symptoms with metoclopramide have been reported with a prevalence of 0.2% of cases, but at the extremes of life it has to increase to 25%. Symptoms begin within the first 24 to 72 hours after administration [11]. The extrapyramidal effects of antiemetics can occur in any clinical form, although the most common reactions involve the axial and predominantly cervicocephalic sectors. Within these extrapyramidal effects there are a large number, but however the most frequent forms of presentation are acute dystonia, tardive dyskinesia and neuroleptic malignant syndrome [12].
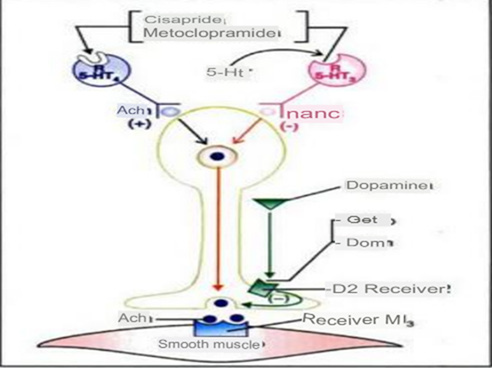
Figure 2: Mechanism of action of metoclopramide.
Acute Dystonia: Acute drug-induced dystonia is an acute movement disorder, which can be painful and distressing. The definition of acute is considered if it occurs within seven days following the start of medication or with elevation of the dose, the different forms of presentation will be spasms or briefly sustained contractions of antagonistic muscle groups, which will result in twisted, unnatural, sustained and repetitive movements or postures [13]. This adverse effect will mainly have focal involvement and affect any muscle group, but with prevalence this involves the head, jaw, neck, mouth and eyes, causing spasmodic torticollis, retrocolis and anterocolis, trismus and dental trauma, among others [14]. As for the treatment of this the first medical will be the suspension of the drug, usually, the dystonia resolves in 24-48 hours. In addition, dystonia responds within 10-20 minutes to anticholinergic agents or antihistamines administered parenterally. In some cases benzodiazepines may be used as adjuvants [15].
Tardive Dyskinesia: Tardive dyskinesia caused by medications (metoclopramide) is mostly associated with chronic use and can compromise feeding, breathing, speech, or ambulation. It presents as a polymorphous involuntary movement disorder. Unlike acute extrapyramidal disorders, on the other hand, subjective symptoms are often described as minimal. The FDA issued a warning about metoclopramide’s risk of causing tardive dyskinesia. The risk of suffering from tardive dyskinesia is increased in patients who remain with metoclopramide for more than twelve weeks [16] in terms of treatment there is no pharmacological treatment, well established and everything is aimed at detecting this pathology early, in order to avoid its sequelae, the use of anticholinergics has been proposed, but these in turn can worsen the symptomatology [14,17].
Neuroleptic Malignant Syndrome: It is characterized by being an acute disorder that affects thermoregulation and neuromotor control. Its etiology is not yet established and can affect any population. The clinical manifestations are caused by the blockade of dopaminergic receptors, causing increased thermogenesis at the hypothalamic level and autonomic instability. The classic presentation consists of 4 symptoms fever, generalized muscle stiffness, alterations of mental state and dysfunction of the autonomic nervous system that presents as hyper or hypotension, increased heart rate, diaphoresis and incontinence of sphincters [17,18]. The patient may also present cardiac alterations such as arrhythmias, renal failure secondary to rhabdomyolysis caused by prolonged muscle contractures that end the death of muscle tissue, which can lead to a state of organ failure with alterations in blood tests, causing more serious complications to the patient [19]. As for the treatment, a multidisciplinary management will be necessary with the protection of the airway, intravenous fluids and correction of the hydro electrolytic disorder in addition to hemodynamic support, the patient in case he needs support with dopamine agonists relaxation and sedation in some more extreme cases with infusion of benzodiazepines, as well as local means for thermoregulation [20].
Discussion
Several authors detail in the literature the correct dosage of metoclopramide to avoid possible adverse effects as follows in adults orally is recommended 10-20mg every 8h, ingested before meals. It also happens when using the parenteral route it is recommended not to exceed 10mg in each dose, and we can use them at intervals of every 6-8 hours. In vomiting due to very emetizing cytotoxics, the doses will be higher. In the pediatric population, the maximum recommended daily dose should not exceed 0.5mg/kg/day, and the recommended doses are: up to 1 year of age, 1mg 2 times a day; 1-3 years, 1mg 2-3 times a day; 3-5 years, 2mg 2-3 times a day; and 5-9 years, 2.5mg 3 times a day. Doses above these have been associated with cases of acute metoclopramide poisoning in most reported cases [21,22]. Likewise, the results obtained by Dr. Ismary Alfonso Orta and company reported that there was a marked trend of adverse reactions due to metoclopramide in those patients whose dose was 30mg daily, considered an average value; on the other hand, in those therapeutic schemes where the dose exceeded 30mg, 63.0% of the cases had direct effects on the CNS, and in the same way, 78.3% of the patients who received doses of 2.5 to 5mg (which corresponded to the pediatric population) presented involvement in this same system [23]. In the study conducted by Jenny Herreño Basabe in the city of Bogota, it shows that the majority of cases reported due to adverse reaction due to drug consumption found that metoclopramide obtained 78.90% that correspond to all cases reported with an absolute value of 202 cases of those reported to the district pharmacovigilance program, data were also reported, although in a smaller percentage when this drug was related to another pharmacological group [10,24].
Conclusion
Metoclopramide is a medication that many health care providers prescribe for the management of different diseases such as certain types of gastroenteritis, migraines, cancer, postoperative states, vomiting, gastrointestinal infections, women in pregnancy. Underestimating the possible adverse reactions that this drug may have on the health of people, in the pediatric population is where the use of this drug is most controversial because most studies reveal that this is one of the most vulnerable population to this type of poisoning due to dosing errors or accidents, its treatment will be aimed at the total suspension of the drug and the mildest forms should resolve in 24-48 hours, associated with the use or not of pharmacological therapy, and the most serious forms for which there is no treatment as such but symptomatic and conservative management of patients is done. All health professionals are invited to know very well the adverse effects of this drug in order to avoid significant sequelae in the lives of patients, so this type of work will be important and should continue to be replicated with medical information every day more updated with respect to the management of these syndromes.
References
- Tibaduiza Mogollón YA, Miranda Diaz AJ (2019) Extrapiramidalismo por antiemé Revista Med 27(2): 65-74.
- Hendren G, Aponte Feliciano A, Kovac A (2015) Safety and efficacy of commonly used antiemetics. Expert Opin Drug Metab Toxicol 11(11): 1753-1767.
- Basch E, Prestrud A, Hesketh P, Kris M, Somerfield M, et al. (2012) Antiemetic Use in Oncology: Updated Guideline Recommendations from ASCO. Am Soc Clin Oncol Educ 12: 532-540.
- Bono J Montilla, Enrique Caro Cruz (1977) Efectos neurológicos inducidos por la metoclopramida. Seminario médico 37: 11-18.
- Aizpuru Galdeano MP (2007) Cuál es el tratamiento más eficaz del reflujo gastroesofágico en lactantes? Hay alguna evidencia de que los productos antirreflujo específicamente comercializados con esta indicación funcionen? Evid Pediatr 3: 110.
- Albano F, Bruzzese E, Spagnuolo M, De Marco G (2006) Antiemetics for children with gastroenteritis: off-label but still on in clinical practice. J Pediatr Gastroenterol Nutr 43(3): 402-404.
- Fedorowicz Z, Jagannath V, Carter B (2011) Antiemetics for reducing vomiting related to acute gastroenteritis in children and adolescents. Cochrane Database Syst Rev 11(9): CD005506.
- Stamer U, Lehnen K, Höthker F, Bayerer B, Wolf S, et al. (2003) Impact of CYP2D6 genotype on postoperative tramadol analgesia. Pain 105(1-2): 231-238.
- Jenny Herreño Basabe (2017) Caracterización De Eventos Adversos Y Problemas Relacionados Con Metoclopramida Reportados Al Programa Distrital De Farmacovigilancia En BogotáC. AL 2017 trabajo de grado, Universidad De Ciencias Aplicadas Y Ambientale.
- Raviña Rubira E (2009) Un viaje a lo largo de la evolución histórica de descubrimiento de fá Universidad de Santiago de Compostela.
- Moos D, Hansen D (2008) Metoclopramide and extrapyramidal symptoms: a case report. J Perianesth Nurs 23(5): 292-299.
- Wittmann O, Sadot E, Bisker Kassif O, Scolnik D, Tavor O, et al. (2016) Neuroleptic malignant syndrome associated with metoclopramide use in a boy: Case report and review of the literature. Am J Ther 23(5): e1246-1249.
- Alhashimi D, Alhashimi H, Fedorowicz Z (2006) Antiemetics for reducing vomiting related to acute gastroenteritis in children and adolescents. Cochrane Database Syst Rev 19(3): CD005506.
- Caroff S, Campbell E (2016) Drug-induced extrapyramidal syndromes: Implications for contemporary practice. Psychiatr Clin North Am 39(3): 391-411.
- Wijemanne S, Jankovic J, Evans R (2016) Movement Disorders from the use of Metoclopramide and other antiemetics in the treatment of migraine. Headache 56(1): 153-161.
- Dsouza R, Mercogliano C, Ojukwu E, Dsouza S, Singles A, et al. (2018) Effects of prophylactic anticholinergic medications to decrease extrapyramidal side effects in patients taking acute antiemetic drugs: A systematic review and meta-analysis. Emerg Med J 35(5): 325-331.
- Zou D, Shao Y, Qin Z, Zhang J, Liu N, et al. (2014) Death due to fulminant neuroleptic malignant syndrome induced by low doses of haloperidol: A rare case. Forensic Leg Med 24: 12-14.
- Tibaduiza Y (2015) Rabdomiólisis en la primera semana de entrenamiento. Reporte de dos casos. Revista Med 23(2): 96-109.
- Reilly T, Kirk M (2007) Atypical antipsychotics and newer antidepressants. Emerg Med Clin North Am 25(2): 477-497.
- Susman V (2001) Clinical management of neuroleptic malignant syndrome. Psychiatr Q 72(4): 325-336.
- Van Patten RA (2015) Síndrome serotoniné Boletín para profesionales. Centro de Información de Medicamentos y Farmacoterapéutica. Servicio de Farmacia. Hospital san Juan de Dios 5: 1-8.
- María Constanza Schell, Benjamín P Parodi (2013) Intoxicación aguda por metoclopramida. Revista de la asociación médica de bahía blanca 23(1).
- Alfonso Orta Ismary, Jiménez López Giset, Chao Cardeso Ashley, Ávila Pérez Jenny (2011) La metoclopramida y sus reacciones adversas sobre el sistema nervioso central. Rev Cubana Med Gen Integr 27(2).
- Juan Carlos Leza Cerro, Ignacio Lizasoain Hernández, María Angeles Moro Sánchez, Antonio Portolés Pérez, Pedro de Lorenzo Fernández, et al. (2018) Velázquez Farmacología Básica y Clínica. In: Juan Carlos Leza Cerro, Ignacio Lizasoain Hernández, María Angeles Moro Sánchez, Antonio Portolés Pérez; Pedro de Lorenzo Fernández, et al. (Eds.)., Editorial Médica Panamericana, spain.
