 Case Report
Case ReportABSTRACT
We present a case of ductal prostate cancer forming a cyst with the untypical symptoms of incontinence and hematuria. The diagnosis was made with partial transurethral resection of the prostate which led to opening of the cyst. After the histologic verification of the cancer hormonal treatment was administered.
Keywords: Prostate Cancer; Gleason Score 4+4;Incontinence; Hematuria
Introduction
Prostatic cysts are relatively uncommon and without typical clinical presentation. That is why urologists generally do not think about them while making the diagnosis of the patients. Very often they are found incidentally during the ultrasound examination and pose significant diagnostic and treatment challenges.
Case Presentation
A 78-years old man presented with symptoms of incontinence and hematuria-from 2years. The hematuria was intermittent, macroscopic and painless, without clots –obviously not profuse because the level of hemoglobin was normal. The incontinence was neither stress nor urge and also not profuse. The digital rectal examination revealed an enlarged prostate-painless, soft and smooth, protruding to the rectum. The ultrasound showed normal kidneys and bladder –below the bladder a cyst was found 50/51mm diameter with thick irregular wall (shown in Figure 1). A normal prostate was visible on some planes with the cyst situated behind and to the left of the prostate. PSA level was 15.8 ng/ml.
MRI (shown in Figure 2) revealed enlarged prostate 80/56/53 mm. and more than 50% of the volume of the prostate was occupied by a cyst (slightly to the left side) with thick irregular wall. The MRI suggested a malignant condition but no PI-RADS evaluation was given. There were no signs of trans-capsular extension of the tumor. Some pelvic lymph nodes were enlarged up to 12 mm. Urethrocystoscopy was performed-nothing abnormal was found. Part of the left lobe was resected and the cyst was opened-the liquid inside was clear, with many papillary growths from the cyst wall. A biopsy from the growths was taken-the pathological result was ductal cancer, Gleason score 4+4. After the biopsy the symptoms (hematuria and incontinence) disappeared and the cyst was invisible on the ultrasound (shown in Figure 3). 1 week later the symptoms appeared again. The ultrasound (shown in Figure 4) revealed that the cyst was again visible, although smaller than before. No treatment was applied and gradually (within several weeks) the incontinence and hematuria disappeared, the cyst was completely invisible on the ultrasound. The patient chose hormonal therapy (LHRH-agonist) for the prostate cancer which is now administered-PSA was 0.58 ng/ml 4 weeks after the start of the therapy.
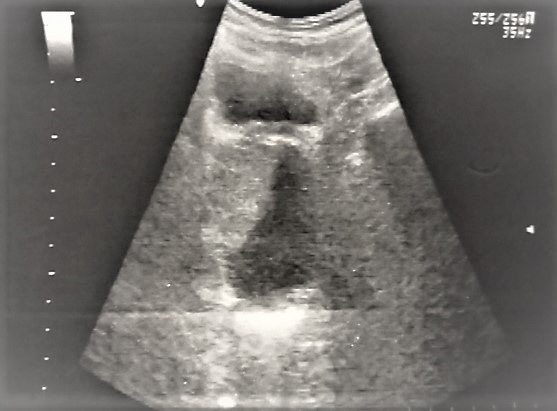
Figure 1: The prostatic cyst at the initial presentation.
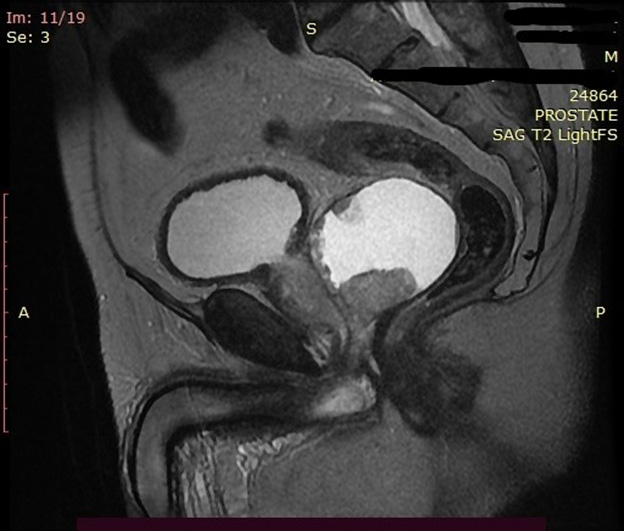
Figure 2: MRI image of the cyst.
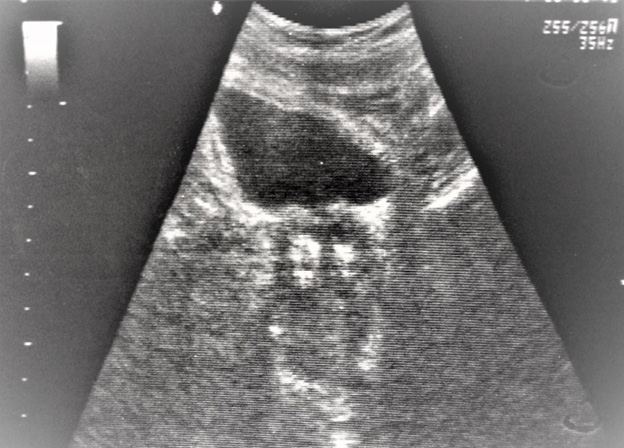
Figure 3: The cyst after the TURP.
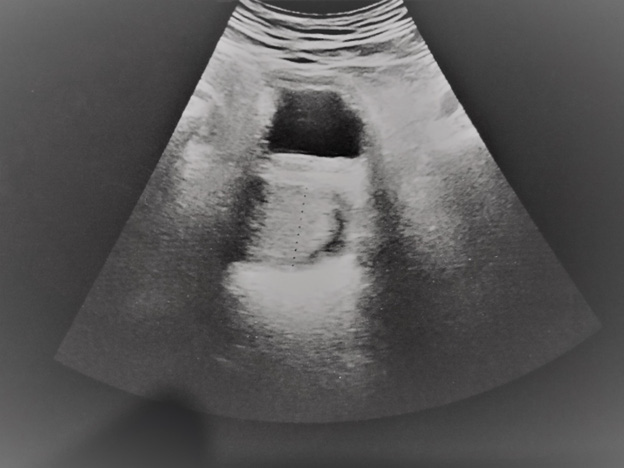
Figure 4: The cyst 1 week after the TURP.
Discussion
The incidence of prostatic cysts can be as high as 7.9%-most of them are benign [1]. Usually they are asymptomatic; the most common presenting symptoms (if there are at all) are usually difficult urination (including retention), frequency and urgency [2]. In our case the patient presented with leakage of clear liquid from the urethra between the normal urinations- the patient called this incontinence but it is also possible that it was a leakage of the intracystic fluid. There was also hematuria-probably also from the intracystic cavity because the cystoscopy showed completely normal urothelium. These symptoms imply a possible connection (although not visible) between the cystic cavity and the urethral lumen. Midline cysts are usually benign and congenital-sometimes associated with infertility [3] – examples include Mullerian duct cysts, prostatic utricle cysts, ejaculatory duct cysts, ductus deferens cysts [4-6]. In our case the cyst was lateral and the patient was elderly. Possible lateral cystic lesions are cystic degeneration of benign prostatic hyperplasia, prostatic retention cyst, seminal vesicle cyst, diverticular prostatitis, prostatic abscess, parasitic prostatic cyst and cystic prostatic carcinoma [7,8].
The ultrasound provided the initial diagnosis of a prostatic cyst and PSA measurement and MRI raised the suspicion that the cyst was malignant – namely the presence of irregular wall with internal enhancing solid components suggests cancer. Unfortunately, from the MRI no PI-RADS assessment was given - probably because of the highly unusual presentation of the tumor. Therapeutic options for managing prostatic cysts include transrectal aspiration with or without sclerotherapy, transurethral marsupialization and open surgery [9-11]. Also, a CT- guided biopsy for histological diagnosis is described in the literature [12]. We opted for a transurethral resection of the prostate because the papillary growths inside of the cyst were considered to be malignant. With opening of the cyst (in fact a transurethral marsupialization) the resectoscope entered the cystic cavity and some papillae were taken for histology. The inracystic fluid was clear which is not typical for carcinomas. The pathological examination initially was inconclusive-second review by a more experienced pathologist was necessary to establish the diagnosis of the tumor.
The pathological result was ductal cancer which is relatively rare (shown in Figures 5-7). Also immunohistochemistry was used (shown in Figure 8) with High-Molecular-Weight cytokeratin-no staining of myoepithelial cells was observed. The literature review showed that in most cases (nine out of ten cases) the pathological finding is acinar-type prostatic adenocarcinoma- only in one case a ductal component was reported [12]. Actually most cases of prostate cancer with cyst formation were pseudocysts with haemorrhage – not true cystic prostatic carcinomas. Only 17% of the cystic tumors were derived from degeneration of a retention cyst [13]. The patient chose hormonal therapy (instead of radical prostatectomy) because of his advanced age. 1 year after the operation PSA is still 0 and on the ultrasound the cyst is invisible – despite the fact that ductal prostate cancer is associated with worse prognosis compared with the typical adenocarcinoma, including overall survival and cancer-specific survival [14].
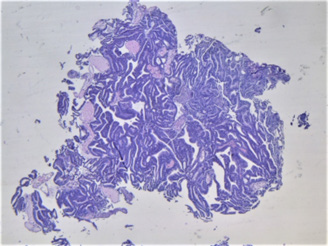
Figure 5: Hematoxylin and eosin staining, x40 magnification.
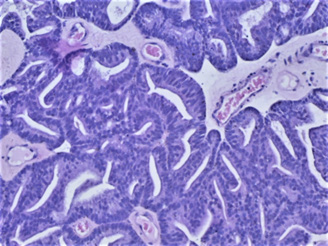
Figure 6: Hematoxylin and eosin staining, x200 magnification.
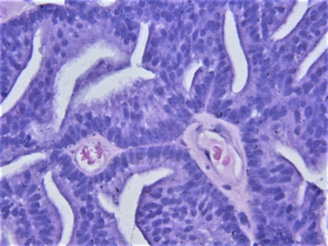
Figure 7: Hematoxylin and eosin staining, x400 magnification.
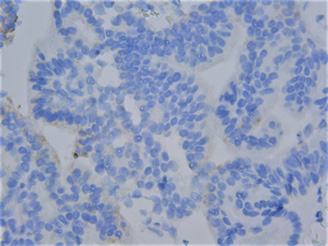
Figure 8: Immunohistochemistry with HMW cytokeratin.
Conclusion
Prostatic cysts are relatively uncommon with varying clinical presentation. Ultrasound is very valuable for the initial diagnosis. PSA and MRI are performed in order to exclude a tumor. In many cases the TURP is a possible treatment and provides the final (pathological) diagnosis.
Statement of Ethics
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Conflict of Interest Statement
The author has no conflicts of interest to declare.
Funding Sources
The author has received no funding.
References
- Hamper UM, Epstein JI, Sheth S, Walsh PC, Sanders RC (1990) Cystic lesions of the prostate gland. A sonographic pathologic correlation. J Ultrasound Med 9: 395-402.
- Issa MM, Kalish J, Petros JA (1999) Clinical features and management of anterior intra urethral prostatic cyst. Urology 54: 923.
- Shebel HM, Farg HM, Kolokythas O, El-Diasty T (2013) Cysts of the lower male genitourinary tract: embryologic and anatomic considerations and differential diagnosis. Radiographics: a review publication of the Radiological Society of North America Inc 33(4): 1125-1143.
- Ishikawa M, Okabe H, Oya T, Hirano M, Tanaka M, et al. (2003) Midline prostatic cysts in healthy men: incidence and transabdominal sonographic findings. AJR Am J Roentgenol 181(6): 1669-1672.
- Schwartz JM, Bosniak MA, Hulnick DH, AJ Megibow, BN Raghavendra (1988) Computed tomography of midline cysts of the prostate. J Comput Assist Tomogr 12(2): 215-218.
- Kim ED, Onel E, Honig SC, Lipschultz LI (1997) The prevalence of cystic abnormalities of the prostate involving the ejaculatory ducts as detected by transrectal ultrasound. International urology and nephrology 29(6): 647-652
- Nghiem HT, Kellman GM, Sandberg SA, Craig BM (1990) Cystic lesions of the prostate. Radiographics 10(4): 635-650.
- Curran S, Akin O, Agildere AM, Zhang J, Hricak H, et al. Endorectal MRI of prostatic and periprostatic cystic lesions and their mimics. AJR Am J Roentgenol 188(5): 1373-1379.
- Saha B, Sinha RK, Mukherjee S, Mitra N (2014)Midline prostatic cyst in a young man with lower urinary tract symptoms. BMJ Case Rep.
- Issa MM, Kalish J, Petros JA (1999) Clinical features and management of anterior intraurethral prostatic cyst. Urology 54: 923.
- Dik P, Lock TM, Schrier BP, ZeijlemakerBY, TA Boon (1996) Transurethral marsupialization of a medial prostatic cyst in patients with prostatitis-like symptoms. J Urol 155: 1301-1304.
- KH Fung, WK Tsang, Philip CH Kwok, WT Lee, KW Tang (2020) Cystic prostatic carcinoma: case report and literature review. Hong Kong Med J 26: 66-69.
- Kim SC, Fujimoto K, Matsumoto Y, M Cho, O Natsume, et al. (2001) A case of prostate cancer with cyst formation. Hinyokika Kiyo 47: 653-656.
- Jiatong Zhou, Jie Ding, Jun Qi (2022) Comparison of typical prostate adenocarcinoma and rare histological variant prostate cancer showed different characteristics and prognosis: a surveillance, epidemiology, and end results database analysis. European urology 82: 152–155.
