 Review Article
Review ArticleAbstract
Obesity is considered an epidemic in the world, has exclusivity in developed countries, but also reaches developing countries like Brazil. It is characterized as excessive accumulation in full extent, which denigrates the state of sweat in individuals through pathophysiological changes directly and indirectly in the metabolic profile and establish chronic inflammation in its carriers. The chronic inflammation process is strongly related to obesity due to the higher production of inflammatory cytokines, which are produced by adipocytes. For the accomplishment of this work the methodology used was the literature review based on national and international scientific articles, as well as books. The articles were searched in the electronic databases Scielo Scientific Electronic Library Online, Inca National Cancer Institute, Google Academic, MedLine Medical Literature Analysis and Retrieval System Online. In conclusion, the correlation result of obesity and chronic inflammation was expected, since the expression of proinflammatory cytokines is increased in individuals with obesity [1-25].
Keywords: Chronic inflammation, Obesity, Inflammatory cytokines, Metabolic syndrome, Cardiovascular complications
Introduction
Obesity is considered an epidemic in the world, has exclusivity in developed countries, but also reaches developing countries such as Brazil. Rising countries are estimated to experience greater increases in the prevalence of such a disease in the 21st century [25- 47]. The consequences of this situation for the health of the world population are calamitous, associated with major socioeconomic impacts. Ferreira [48]. Several countries that are still developing already have a posture similar to that of developed countries, such that the fractions of obesity overlap the fractions of malnutrition. It has been observed that in such countries the equivalence of obesity with higher socioeconomic status had no documented notoriety as compared to the First World a decade or two ago. As a result, several studies conducted since the 1990s questioned the relationship of obesity and whether it was a disease exclusively linked to better socioeconomic conditions. Monteiro et al. [34].
This study addresses obesity and its relationship with chronic inflammation. Therefore, it concomitantly addresses the varied aspects of this state of comorbidity, which are the pathophysiology of the Metabolic Syndrome, the characteristics of obesity, the complications directly and indirectly caused by the disease. excessive visceral obesity, epidemiology, the nutritional pattern of patients with metabolic syndrome, so that new diagnostic patterns for such pathological status are defined and developed by analysis of these aspects. Metabolic alterations remain as research targets because they are constant and increasing variables at any social level, therefore, the present work aims to promote an update on such variations, therefore, this requalification should be performed primarily aiming at the diagnostic criteria and the physiomorphological variations considered. as new principles in determining and assessing the impacts of metabolic syndrome and obesity directly and indirectly on its carriers, as they are highly prevalent and result in cardiovascular complications, which in turn are the leading causes of death in the world [49-61].
The pathological state of obesity can promote direct and indirect changes in the metabolic profile and establish chronic inflammation in its carriers. Therefore, understanding this state of comorbidity will improve the diagnosis and treatment of obesity. Today obesity is a chronic disease that can be considered epidemic worldwide, based on the relationship with metabolic changes and complications caused by assessing potential damage, obesity then became a public health priority, so what relationship of obesity with chronic inflammation? This study addresses the characteristics of obesity and its epidemiology, inflammatory adipokines and their characteristics, and complications directly and indirectly caused by excessive visceral obesity.
Methodology
The study is a review of narrative literature, was based on secondary publications before a reading of the abstracts found with publication in monographs, books, magazines, academic articles, dissertations. The data sources were made through national and international websites, SciELO Scientifi Electronic Library Online, MEDLINE Medical Literature Analysis and Retrieval System Online, PubMed US National Library of Medicine, Google Academic, among other sources that may help. in the enrichment of work. The descriptors used were: Metabolic Syndrome X SMX, obesity, chronic inflammation, cardiovascular complications. The elaboration of the present study was based on the data sources mentioned above. This review will serve as a basis for further studies focusing on obesity and inflammatory cytokines. In the research of the studies that theoretically based this work the following keywords were used: metabolic syndrome, cytokines, chronic inflammation and epidemiology of obesity. As inclusion criteria were used monographic works, theses, books and scientific articles that were found in full text format and free of charge in electronic databases and were used works published from 1987 to 2017 and that were in Portuguese, English and Spanish.
Obesity
Features of Obesity
Obesity is characterized as excessive accumulation in full extension, which denigrates the sweating state in individuals through pathophysiological changes Ferrari [8] but the degree of excess fat and its body distribution, along with the changes caused are variable. among obese individuals WHO, 1998. The group of NCDs Non-Communicable Chronic Diseases has obesity as its member. The diseases of such a group, when directed at their actual definitions, are difficult to conceptualize, regardless of how it is developed. However, they can be characterized by their various factors directly or indirectly involved Kolotkin et al. [57]. Having obesity as a disease, it has several causes and is also a result of genetic, metabolic, social, behavioral and cultural factors Brazil, Ministry of Health [7]. As prevalence in these cases, the abuse of caloric intake associated with sedentary lifestyle, excess calories that are not used, are now stored in adipose form fatty tissue, thus causing the positive energy balance, which is defined as the differential between the acquired energy and its use as an energy source in the execution of vital functions and various activities Francischi et al. [16]. Therefore, it is considered as positive when the energy activity that is acquired overlaps the expenditure, which varies between individuals Schieri et al. [49], Gigante [18], Motta et al. [35].
Genetic factors may be related to efficiency in the utilization, storage and direction of ingested nutrients, energy expenditure, exclusively basal metabolism BMR, appetite control and eating behavior Schieri et al. [49], Gigante [18]. The disease may be related to some endocrine disorders, such as hyperthyroidism and disorders of the hypothalamus, but such causes represent less than 1% of obese individuals. In addition, people who indicate parental maternal / paternal obesity are almost twice as likely to develop obesity as those who do not have obese parents Motta et al. [35]. External factors such as social, economic and cultural are included when it comes to determining obesity, highlighting the new role of women in society and its introduction into the labor market. Such factors seem to play a role in the development of obesity, urban agglomeration and reduced physical exertion and, as a result, the reduction of energy expenditure in the professional and daily routine and the growing food industry Marinho et al. [29]. There are also other factors associated with obesity, such as changes in data moments of life, situations of violence, psychological factors, some drug treatments, smoking cessation, alcoholism and drastic reduction of physical activity Mendonça & Anjos [31], Motta et al. [35].
Nutritional Pattern of Obese Individuals
According to the literature, not only total energy intake and expenditure promote the regulation of the amount of energy in body stocks Flatt [14,15]. But the energy balance of each macronutrient strictly influences the adjustment of its consumption with its oxidation and vice versa, and maintaining the equilibrium state. The balance between nitrogen and carbohydrates is easily promoted through the ability to adjust the amino acid and glucose oxidation parameters of the body correlated with food intake Flatt [14]. When referring to fat, such adjustment occurs with difficulty in accuracy, therefore, if promoted an increase in the intake of this fraction, there is no stimulus of equal proportion to oxidation. In addition, dietary lipid has a high efficiency parameter in storing it as adipose tissue with a percentage around 96% WHO [58]. Therefore, increased intake promotes positive lipid balance, and as a result, there is an increase in adipose tissue. Metabolic syndrome X is defined by a set of risk factors, which are commonly related to increased insulin resistance and visceral obesity. These factors are connected by biochemical, physiological, clinical and metabolic aspects, which promote a direct increase in the risk of developing Type 2 Diabetes Mellitus DM2 and Cardiovascular Diseases CVD. It has variable incidence in diverse populations according to ethnicity, age, gender and region urban or rural, and according to the diagnostic criterion. According to the International Diabetes Federation - IDF 2005, 25% of the adult population has the syndrome IDF [27], Bhatt H et al. [5]. According to diagnostic criteria, such as the EGIR - European Group for the Study of Insulin Resistance 1991, the AACE - American Association of Clinical Endocrine Logists 2003 and the IDF 2005, however, the National Cholesterol Education Program - Adult Treatment Panel III 2001 is the diagnostic criterion recommended by the First Brazilian Metabolic Syndrome Directive IDBSM, 2005. Such diagnostic criteria included insulin resistancerelated RI blood glucose deviations, increased BMI values, elevated triglyceride levels and decreased HDL-C high density lipoprotein, and high blood pressure Won et al. [57].
In the recent literature, there is a consensus that at least six criteria show the presence of MS: obesity, waist circumference WC> 102cm in males or> 88cm in females, IR fasting glucose above 100mg/dl, high triglyceride levels > 150mg/dl and low HDL-C levels <40mg/dl in males or <50mg/dl in females, presence of hypertension 130/85 mm Hg and a proinflammatory and prothrombotic state. A carrier is defined as an individual who has three or more of the factors presented above Bonomini et al. [6], Coffman & Richmond-Bryant [10], Grundy et al. [20], Abella et al. [1]. Even so, it is not necessarily necessary to have a high BMI to have MS present, so it is possible to define that obesity is a risk factor, but not present in all patients. Indeed, studies show that MS can also be present in other pathologies, such as liver steatosis, cancer, depression, rheumatic and respiratory diseases Martocchia A et al. [31], Abella V et al. [1].
Obesity has been considered as a chronic and epidemic disease, as it has been shown to be rapidly expanding and prevalent in recent decades, regardless of whether the country is developed or developing, and is related to a high rate of morbidity and mortality Oliveira et al. [9]. One study describes that there is a possibility that its advancement reaches 10% of such countries and that practically 33.5% of the American population is overweight FRANSCISCHI et al. 2000. However, obesity is uncommon in African and Asian countries, with a higher prevalence in the urban population than the rural population. In regions with advanced economies, prevalence may be as high as industrialized countries World Health Organization - WHO [58]. According to data from the World Health Organization 1998, they indicate a contrast between African regions and industrialized nations, where the main aspects analyzed are malnutrition and food security. In the American continent, studies define that the parameter for obesity is high for both sexes, both in developed and in developing countries. In the European continent, there was an increase of 10% to 40% in the parameter of obesity in most countries, mainly England, with such an increase being more than double between the 80’s and 90’s. In the West region Pacific, which includes Australia, Japan, Samoa and China, was also evidenced an increase in the prevalence of obesity however, it is noteworthy that China and Japan, despite having an increase in obesity in contrast to developed countries, had the lowest. prevalence rates, which are 0.36% for women and 0.86% for men aged 20-45 years in 1991 in china, 1.8% for men and 2.6% for women over 20 in 1993 in Japan Monteiro et al. [34].
The most significant data on the prevalence of obesity globally are provided by the Monitoring of Trends and Determinants in Cardiovascular Diseases WHO MONICA study. According to the same, BMI parameters between 25 and 30 are responsible for the largest impacting fraction of overweight on certain comorbidities associated with obesity. The same example illustrates that about 60% of men and 77% of women with Non-Insulin Dependent Diabetes Mellitus DM-NID, can theoretically prevent the disease if they have a BMI less than or equal to 25 WHO [58].
Inflammatory Adipokines
Adipokines are a group of substances that have their expression and secretion promoted by adipose tissue. However, the action of most of them is not clearly defined, there may be claims that are intrinsically related to excess and distribution of body fat. Higher production of proinflammatory cytokines occurs through adipocytes. From this point on, it is understood that there is a predicted relationship between higher secretion and high levels of cytokines in obese individuals, which predisposes to the risk of developing metabolic syndrome. VOLP et al. 2008. The most relevant pro-inflammatory cytokines are: interleukin-6 IL-6, tumor necrosis factor-α TNF-α, interleukin-8 IL-8, interleukin-1β IL -1β and CD40 and CD40L WU JT & WU JL, 2006.
Interleukin-6
IL-6 is a proinflammatory cytokine, which is involved in the development of hyperinsulinemia and MS, as it plays a major role in carbohydrate and lipid metabolism by promoting lipolysis through lipoprotein lipase LPL. and increased release of glycerol and free fatty acids, and reduced expression of insulin-1 receptor IRS-1 and GLUT-4 substrate in muscle and liver tissues Rexrode et al. [45]. Being a pleiotropic cytokine, IL-6 performs a succession of functions on cellular and humoral immune effects related to inflammation, individual defense and tissue damage Francisco et al. [18]. And as the central intermediate of the acute phase response and major procoagulant cytokine, it defines the elaboration and elevation of liver-stimulated plasma concentrations of fibrinogen, which is a serum amyloid protein A SAA, especially C-reactive protein PCR Willerson & Ridker [55]. Individuals with high CRP levels > 1.35μg/ mL also demonstrated increased IL-6 values 3.22pg/mL when found with individuals with low CRP levels <1.35μg/mL. , which demonstrated reduced IL-6 values 1.35ng/mL Volp et al. [3]. Such action is related, in part, as a result of CRP stimulation by IL-6 Yudkin et al. [60].
IL-6 has its production and secretion through endothelial cells, smooth muscle cells, monocytes and macrophages and is capable of contributing to the evolution of atherosclerotic injury due to its paracrine, autocrine and endocrine effect Francisco et al. [18]. It has its secretion mainly promoted by adipocytes, specifically visceral adipose tissue Rexrode et al. [45]. Serum IL-6 levels are closely associated with waist circumference Rexrode et al. [45], demonstrating that individuals with android obesity have a higher chance of developing metabolic syndrome, such effect is increased in obesity due to higher accumulation of body fat.
Tumor Necrosis Factor-α TNF-α
This factor is a cytokine that has autocrine, paracrine and endocrine actions Montague et al. [33], Ruan & Lodish [48]. It has its action on adipocytes, providing a regulatory function in the accumulation of adipose tissue by inhibiting lipogenesis, reducing the expression of LPL, GLUT-4 and acetyl-CoA synthetase, also with increased lipolysis Montague et al. [33], RNAER, 1995. Obese individuals have strong inverse interdependence between TNF-α and glucose metabolism Winkler et al. [56]. The effect is produced as a result of TNF-α suppression of insulin signaling, reducing IRS- 1 phosphorylation and insulin kinase receptor P13K action. This accomplishment reduces the synthesis and translocation of glucose carrier GLUT-4 to the same membrane with consecutive reduction in insulin-mediated glucose uptake by cells. Decreased peripheral insulin sensitivity leads to increased glycogenesis and hepatic and decreases glucose clearance by skeletal muscle and adipose tissue, configuring a hyperinsulinemic state Arner [4], Hsueh & Law [25]. As a result of its pleiotropic biological activity, TNF-α is involved in the inflammatory process, as it plays a major role in the cytokine cascade, in addition to stimulating the synthesis of other cytokines Francisco et al. [18]. Like IL-6, TNF-α is the center of acute phase response mediation as it determines the formation and increase of plasma concentrations promoted by fibrinogen liver, SAA, plasminogen-1 activator inhibitor PAI-1 and, exclusively, PCR Francisco et al. [18], Willerson & Ridker [55], Yudkin et al. [60]. In addition, TNF-α provides for IL-6 expression in adipose tissue and provides for endothelial expression of adhesion molecules Darval et al. [11].
Interleukin-1β IL-1β
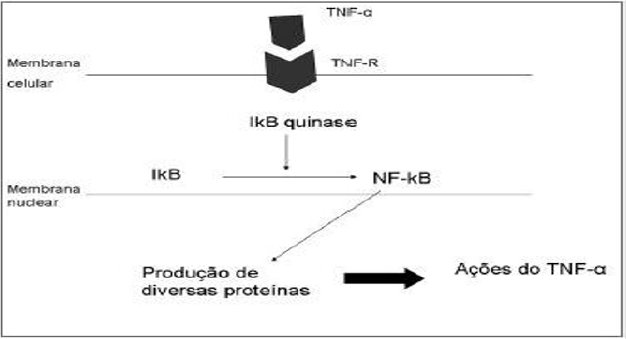
Figure 1: NF-κβ gene activation scheme (VITALE & RIBEIRO, 2007).
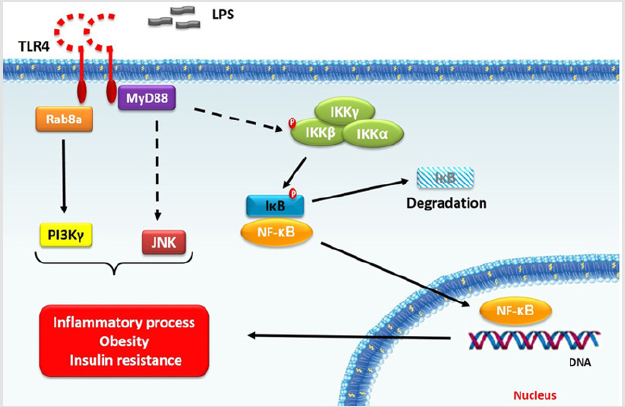
Figure 2: Once activated, IKK-β phosphorylates IκB protein, which, in turn, release NF-\ complex (Cavalcante Silva, 2015).
The IL-1 cytokine category contains various pro-inflammatory cytokines, which are involved in the atherogenic process and metabolic syndrome. Thus, IL-1β belongs to the group of IL- 1, and normally its production is exerted by monocytes and macrophages, however, can also be produced by other cells, such as endothelial cells, smooth muscle cells and activated platelets. This cytokine promotes transcriptional activation of the NF-κβ gene for expression of adhesion bodies and cytokines. In addition, it increases the expression of endothelial adhesion corpuscles, facilitating the association of other inflammatory cells of the activated endothelium Francisco et al. [18]. Below is an image, which contains an activation scheme of the NF-κβ gene: Together with TNF-α, it stimulates IL-6 production by smooth muscle cells and elevates the expression of macrophages, platelet-derived growth factor PDGF and associated fibroblast growth factor FGF. with the chaining of the atherosclerotic inflammatory process Volp et al. [3] (Figures 1 & 2).
Interleukin-18 IL-18
IL-18 is another participant cytokine of the IL-1 group, and requires special relevance regarding its activity in the atherogenic process. Proinflammatory cytokines, such as IL-1β, IL-6 and TNF-α, boost macrophage expression of IL-18. Through its receptor expressed on 1-T-helpers lymphocytes, endothelial cells, smooth muscle cells and macrophages, IL-18 promotes the secretion of IL-6, TNF-α, IL-1β and ICAM-endothelial adhesion corpuscles. 1 and VCAM-1 Francisco et al. [18]. Therefore, IL-18 is also a proinflammatory cytokine with pleiotropic action, which is linked to major regulatory functions in the immune response and is classified as an inflammatory marker Hung et al. [26]. Among other roles, IL-18 performs, in particular, human T-cell chemotaxis, enabling its recruitment into the plaque. Moreover, IL-8 seems to induce the expression of several metalloproteinases, which can weaken the fibrous cap of atherosclerotic lesion, converting a vulnerable plaque Francisco et al. [18].
CD40 and CD40L
CD40 is a membrane protein that constitutes the TNF receptor group, and CD40L is a constituent of the TNF group, both coexpressed by macrophages, T lymphocytes, platelets, endothelial cells and smooth muscle cells Francisco et al. [18]. In such a way, they are incorporated as new inflammatory markers Guldiken et al. [21]. CD40L is presented in soluble form sCD40L and as a transmembrane protein. Serum levels of sCD40L represent CD40 / CD40L system activation. Such a system has been widely implicated in the pathophysiology of atherosclerosis, from the early atherogenic process to the late process of thrombotic complications. Regarding the functions, the system plays a variety of proinflammatory and prothrombotic effects, such as: stimulation of free radical production ROS in endothelial cells, which antagonize nitric oxide production, induction of adhesion corpuscles CAMs expression in smooth and endothelial muscle cells, stimulation of expression of proinflammatory cytokines and chemokines, increased expression of metalloproteinases, making atherosclerotic plaque more fragile, induction of endothelial tissue factor expression and smooth muscle cells, promoting increased thrombogenic potential of plaque, and participation in platelet activation.
In this sense, it has been shown that CD40 is expressed from the platelet surface, and binding causes platelet activation, which promotes thrombus formation Francisco et al. [18], Wu & Wu. [59].
Complications Directly Caused by Excessive Visceral Obesity
Abdominal obesity causes mononuclear leukocytes lymphocytes and monocytes to be induced to secrete inflammatory cytokines such as IL-1, IL-6, IL-8, TNF-a tumor necrosis alpha and TGF-b factors. transformed growth factor beta Nicklas et al. [39]. The accumulation of visceral fat promotes increased hypersensitivity of adipose tissue to glucocorticoids cortisol, cortisone, etc., which promote greater capacity for arterial vasoconstriction, which is consequently related to hypertension in insulin resistant patients, obesity and SM Walker et al. [52], Whorwood et al. [53]. Excess glucocorticoids stimulate glucose-6-phosphatase, which promotes a greater release of glucose from pancreatic cells and other tissues, such as the liver and muscle, into the bloodstream, thus triggering hyperglycemic and resistance states. tissue to insulin action, thus, another aspect of MS Nambi V et al. [37]. Long-term hyperglycemia promotes increased insulin dispersion, providing a hyperinsulinemic state that, when added to visceral adipose tissue glucocorticoid hypersecretion, promotes negative feedback, which will inhibit pancreatic insulin secretion Ling et al. [29] and contributing to resistance to this hormone in MS and diabetes mellitus type 2 Wajchenberg et al. [51].
Still highlighting the complications caused by the accumulation of visceral fat, its existence increases the risk of non-alcoholic fatty degeneration of the liver, since it promotes increased lipolysis and synthesis of thyroglobulin TG from glucose. Thus, as a consequence, there is an increase in TG by hepatic dispersion to the blood, as well as an increase in its serum levels. Being excess thyroglobulin in the blood is also one of the aspects of MS Nambi et al. [37], promotes a decrease in hepatic HDL secretion and triggers changes in blood viscosity ZIEGLER, 2001, favoring platelet aggregation Osmancik et al. [41] and the risk of thrombosis. Concomitantly, excess thyroglobulin promotes the secretion of very low density lipid VLDL and small, dense low density lipid LDL particles which are oxidized and readily phagocytized by arterial wall macrophages Ziegler [61], Osmancik et al. [41], thus forming foamy deposits Deedwania [12], which progressively lead to lipid lesions or striations until the formation of also lipid aggregates plaques in atherogenic development Osmancik et al. [41], Deedwania [12].
The glycosylation that occurs in diabetes mellitus and MS promotes changes in apoB apolipoprotein B, which involves LDL, allowing it to be phagocytized more easily by macrophages contained in the vascular wall Nesto [38]. However, the presence of visceral adipose tissue induces fibrinogen secretion through the liver, also to serum amyloid protein A and PCR C-reactive protein Nicklas et al. [39], which are also inflammatory indicators of cardiovascular risk in the liver. SM Pearson et al. [42]. For the cardiovascular risk diagnostic parameter, the following CRP values presented in the table below can be adopted Pearson et al. [42]: The decrease in blood vessel caliber is due to atherosclerosis, which promotes increased blood pressure. In MS there is an increase in angiotensin, sodium retention, reduced levels of vasodilation factor derived from endothelium - nitric oxide - and increased levels of endothelin-1 vasoconstrictor peptide, factors that make possible the presence of hypertension in MS and in obesity Reaven [44]. In addition, there is an increase in blood coagulation systems, which consecutively increases the risk of thrombosis Nesto, [38], Nicklas et al. [39], Hermsdorff et al. [24], Reaven [44]. other alterations, such as the synthesis of fibrinogen and plasminogen inhibitor factor PAI-1. Therefore, thrombosis aggravates the atherogenic process and induces vascular narrowing which may result in hypertension.
Complications Indirectly Caused by Excessive Visceral Obesity
According to what has been described, there is an inversion in the relationship between TG and HDL serum levels in MS Nambi et al. [37], Ziegler [61], Reaven [44]. Therefore, commonly those with MS and obesity, practice little physical activity, ie, are sedentary, have lower HDL levels Iglseder et al. 2005. In contrast, regular aerobic exercise activity contributes to the control of body weight, RR heart rate, increased HDL levels and reduced carotid artery thickness Nordstrom CK [40]. Chronic hyperinsulinemia, insulin resistance and hyperglycemia favor the permanence of elevated serum glucose levels. Therefore, the excess of hexoses undergoes biochemical reactions, which undergo conjugation with free amino groups -NH2 in proteins, lipids and nucleic acids for the final formation of Age advanced glycosylation products, the glycated hemoglobin Hba1c Peppa et al. [43]. They are also related to albuminuria, glomerulomegaly, and glomerulonecrosis Tuttle, 2005. Hyperinsulinemia is due to chronic renal failure, it is an indicator of renal impairment degree of injury in MS Nambi et al. [37], Reaven et al. [44]. Obese individuals are more likely to be affected by obstructive sleep apnea, which in turn is related to an increased risk of uncontrolled blood glucose. It was defined as a risk factor after a critical literature review Wiernsperger et al. [54] (Chart 1).
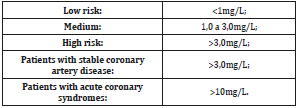
Chart 1: Reference values as a diagnostic parameter for cardiovascular risk.
Conclusion
Adipose tissue dynamically secretes various pro-inflammatory cytokines. Therefore, the correlation between the degree of obesity and chronic inflammation is expected, however, several comparisons between the diagnostic components of metabolic syndrome and the markers of inflammation can come about regardless of the degree of obesity. I have their highest serum levels. according to the superiority of the fat body mass. However, the expressiveness between markers of chronic inflammation with obesity and other aspects related to MS can be similar, regardless of whether the individual is healthy or not, and also in normal or overweight people. There are a range of external factors that should be taken into account as determinants of inflammatory status, such as physical activity levels and dietary patterns, assessed in parallel with biochemical, anthropometric and body constitution values. The findings presented in this review have important clinical relevance. The process of chronic inflammation has great complexity in its reaction, because the various markers mentioned perform numerous functions and follow various metabolic pathways. Therefore, the need for further research on the inflammatory process to identify new inflammatory processes, reference and also risk levels, and cutoff, being more specific with the Brazilian population.
References
- Abella V, Scotece M, Conde J, Veronica Lopez, Veronica Lazzaro, et al. (2014) Adipokines, metabolic syndrome and rheumatic diseases. J Immunol pp. 343-746.
- Amelio F Godoy Matos, Ivan C Cruz, Rafael da Costa, Wellington S Silva Junior, Brazilian Adipokines Study Group (2014) Adipocinas: uma visão geral dos seus efeitos metabó Revista HUPE Rio de Janeiro 13(1): 54-60.
- Ana Carolina Pinheiro Volp, Rita de Cassia G Alfenas, Neuza Maria Brunoro Costa, Valeria Paula Rodrigues Minim, Paulo Cesar Stringueta, et al. (2008) Capacidade dos Biomarcadores Inflamatórios em Predizer a Síndrome Metabó Arq Bras Endrocrinol Metab 52(3).
- Arner P (1995) Differences in lipolysis between human subcutaneous and omental adipose tissues. Ann Med 27(4): 435-438.
- Bhatt H, Safford M, Glasser S (2015) Coronary heart disease risk factors and outcomes in the twenty-first century: findings from the reasons for geographic and racial differences in stroke (REGARDS) study. Curr Hypertens Rep 17(4): 541.
- Bonomini F, Rodella LF, Rezzani R (2015) Metabolic syndrome, aging and involvement of oxidative stress. Aging Dis 6(2): 109-120.
- Ministerio da saude (2006) Epidemiologia: relevância do problema e conceito e classificaçã Cadernos de Atenção Básica n.º12. Série A. Normas e Manuais Técnicos p. 16-26.
- Carlos Kusano Bucalen Ferrari (2007) Atualização: Fisiopatologia e Clínica da Síndrome Metabó Arquivos Catarinenses de Medicina 36(4).
- Cecilia Lacroix de Oliveira, Marco Tulio de Mello, Isa de Padua Cintra, Mauro Fisberg (2004) Obesidade e síndrome metabólica na infância e adolescê Rev Nutr Campinas 17(2): 237-245.
- Coffman E, Richmond Bryant J (2015) Multiple biomarker models for improved risk estimation of specific cardiovascular diseases related to metabolic syndrome: a cross-sectional study. Popul Health Metr 13: 7.
- Darvall KAL, Sam RC, Silverman SH, Bradbury AW, Adam DJ (2007) Obesity and thrombosis. Eur J Vasc Endovasc Surg 33(2): 223-233.
- Deedwania PC (2003) Diabetes and vascular disease: common links in the emerging epidemic of coronary artery disease. Am J Cardiol 91(1):68-71.
- Dengel DR, Goldberg AP, Mayuga RS, Kairis GM, Weir MR (1996) Insulin resistance, elevated glomerular filtration fraction, and renal injury. Hypertension 28: 127-132.
- Flatt JP (1987) Dietary fat, carbohydrate balance, and weight maintenance: effects of exercise. Am J Clin Nutr 45(1): 296-306.
- Flatt JP (1995) Use and storage of carbohydrate and fat. Am J Clin Nutr 61(4): 952S-959S.
- Francischi RPP, Pereira LO, Freitas CS, Klopfer MM, Santos RC, et al. (2000) Obesidade: atualização sobre sua etiologia, morbidade e tratamento. Rev Nutr 13(1): 17-28.
- Francisco G, Hernandez C, Simo R (2006) Serum markers of vascular inflammation in dyslipidemia. Clin Chim Acta 369(1): 1-16.
- Gigante DP, Barros FC, Post CLA, Olinto MTA (1997) Prevalência de obesidade em adultos e seus fatores de risco. Rev Saúde Pública 31(3): 236-246.
- Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, et al. (2005) Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 112(17):2735-2752.
- Guldiken S, Demir M, Arikan E, Turgut B, Azcan S, et al. (2007) The levels of circulating markers of atherosclerosis and inflammation in subjects with different degrees of body mass index: soluble CD40 ligand and high-sensitivity C-reactive protein. Thromb Res 8(2): 89-95.
- Han TS, van Leer EM, Seidell JC, Lean MEJ (1995) Waist circumference action levels in the identification of cardiovascular risk factors: prevalence study in a random sample. BMJ 311(7017): 1401-1405.
- Hayden MR, Tyagi SC (2005) Isolated low high density lipoprotein-cholesterol (HDL-C): implications of global risk reduction. Case report and systemic scientific review. Cardiovasc Diabetol 4: 1.
- Hermsdorff HHM, Monteiro JBR (2004) Gordura visceral, subcutânea ou intramuscular: onde está o problema? Arq Bras Endocrinol Metab 48(6): 803-811.
- Hsueh WA, Law R (2003) The central role of fat and effect of peroxisome proliferator-activated and cardiovascular disease. Am J Cardiol 92(4A): 3J-9.
- Hung J, McQuillan BM, Chapman CML, Thompson PL, Beilby JP (2005) Elevated interleukin-18 levels are associated with the metabolic syndrome independent of obesity and insulin resistance. Arterioscler Thromb Vasc Biol 25(6):1268-1273.
- (2005) International Diabetes Federation. The IDF consensus worldwide definition of the metabolic syndrome.
- Kolotkin RL, Crosby RD, Kosloski KD, Williams GR (2001) Development of a brief measure to assess quality of life in obesity. Obes Res 9(2): 102-111.
- Ling ZC, Khan A, Delauny F, Davani B, Ostenson CG, et al. (1998) Increased glucocorticoid sensitivity in islet betacells: effects on glucose 6-phosphatase, glucose cycling and insulin release. Diabetologia 41(6): 634-639.
- Marinho SP, Martins IS, Perestrelo JPP, Oliveira DC (2003) Obesidade em adultos de segmentos pauperizados da sociedade. Rev Nutr 16(2).
- Martocchia A, Stefanelli M, Falaschi GM, Toussan L, Ferri C, et al. (2015) Recent advances in the role of cortisol and metabolic syndrome in age-related degenerative diseases. Aging Clin Exp Res 28(1): 17-23.
- Mendonca CP, Anjos LA (2004) Aspectos das práticas alimentares e da atividade física como determinantes do crescimento do sobrepeso/obesidade no Brasil. Cad Saúde Pública 20(3).
- Montague CT, Prins JB, Sanders L, Zhang J, Sewter CP, et al. (1998) Depot -related gene expression in human subcutaneous and omental adipocytes. Diabetes.
- Monteiro CA, Conde WL (1999) A tendência secular da obesidade segundo estratos sociais: nordeste e sudeste do Brasil, 1975-1989-1997. Arq Bras Endocrinol Metabol 43(3).
- Monteiro CA, Moura EC, Conde WL, Popkin BM (2004) Socioeconomic status and obesity in adult populations of developing countries: a review. Bull WorldHealth Org 82(12): 940-946.
- Motta DG, Peres MTM, Calcada MLM, Vieira CM, Tasca APW, et al. (2004) Consumo alimentar de famílias de baixa renda no município de Piracicaba/SP. Saúde Rev.
- Nambi V, Hoogwerf BJ, Sprecher DL (2002) A truly deadly quartet: obesity, hypertension, hypertriglyceridemia, and hyperinsulinemia. Clev Clin J Med 69(12): 985-989.
- Nesto RW, Rutter MK (2002) Impact of the atherosclerotic process in patients with diabetes. Acta Diabetol 39(2): S22-28.
- Nicklas BJ, You T, Pahor M (2005) Behavioral treatments for chronic systemic inflammation: effects of dietary weight loss and exercise training. Can Med Assoc J 172(9): 1199-1209.
- Nordstrom CK, Dwyer KM, Merz NB, Shircore A, Dwyer JH (2003) Leisure time physical activity and early atherosclerosis: The Los Angeles Atherosclerosis Study 115(1): 19-25.
- Osmancik PP, Bednar F, Mocikova H (2007) Glycemia, triglycerides and disease severity are best associated with higher platelet activity in patients with stable coronary artery disease. J Thromb Thrombol 24(2): 105-107.
- Pearson TA, Mensah GA, Alexander RW, Anderson JL, Cannon RO, et al. (2003) Markers of inflammation and cardiovascular disease. Application to clinical and public health practice: a Statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association. Circulation 107(3): 499-511.
- Peppa M, Uribarri J, Vlassara H (2003) Glucose, advanced glycation end products, and diabetes complications: what is new and what works. Clin Diabet 21(4): 186-187.
- Reaven G (2002) Metabolic syndrome: Pathophysiology and implications for management of cardiovascular disease. Circulation 106(3): 286-288.
- Rexrode KM, Pradhan A, Mansos JE, Buring JE, Ridker PM (2003) Relationship of total and abdominal adiposity with CRP and IL-6 in women. Ann Epidemiol 13(10): 674-682.
- Ribeiro Filho FF, Faria AN, Kohlmann O, Ajzen S, Ribeiro AB, et al. (2001) Ultrasonography for the evaluation of visceral fat and cardiovascular risk. Hypertension 38: 713-717.
- Rodrigo Faller Vitale, Fernando de Andrade Quintanilha Ribeiro (2007) O papel do Fator de Necrose Tumoral Alfa (TNF-α) no processo de erosão óssea presente no colesteatoma adquirido da orelha mé Revista Brasileira de Otorrino laringologia. Janeiro/Fevereiro 73(1): 123-127.
- Ruan H, Lodish HF (2003) Insulin resistance in adipose tissue: direct and indirect effects of tumor necrosis factor-alfa. Cytokine Growth Factor Rev 14(5): 447-455.
- Sandra Roberta Gouvea, Ferreira (2006) A obesidade como epidemia: o que pode ser feito em termos de saúde pública? Obesity epidemics: what can be done in terms of public health? Einstein 4(1): S1-S6.
- Sichieri R, Coitinho PC, Leao MM, Recine E, Everhart J (1994) High temporal, geographic and income variation in body mass index among adults in Brazil. Am J Public Health 84(5): 793-798.
- Wajchenberg BL, Giannella Neto D, Silva MER da, Santos RF (2002) Depot-specific hormonal characteristics of subcutaneous and visceral adipose tissue and their relation to the metabolic syndrome. Horm Metab Res 34(11-12): 616-621.
- Walker BR, Phillips DIW, Noon JP, Panarelli M, Andrew R, et al. (1998) Increased glucocorticoid activity in men with cardiovascular risk factors. Hypertension 31(4): 891-895.
- Whorwood CB, Donovan SJ, Flanagan D, Phillips DIW, Byrne CD (2002) Increased glucocorticoid receptor expression in human skeletal muscle cells may contribute to the pathogenesis of the metabolic syndrome. Diabetes 51(4):1066-1075.
- Wiernsperger N, Nivoit P, Bouskela E (2006) Obstructive sleep apnea and insulin resistance: a role for microcirculation? Clinics 61(3): 253-266.
- Willerson JT, Ridker PM (2004) Inflammation as a cardiovascular risk factor. Circulation 109(21):II2-10.
- Winkler G, Kiss S, Ketszthelyi L, Sapi Z, Ory I, et al. (2003) Expression of tumor necrosis factor (TNF-alfa) protein in the subcutaneous and visceral adipose tissue in correlation with adipocyte cell volume, serum TNF-alfa, soluble serum TNF-receptor-2 concentrations and C-peptide level. Eur J Endocrinol 149(2): 129-135.
- Won KB, Chang HJ, Niinuma H, et al. (2015) Inverse association between central obesity and arterial stiffness in Korean subjects with metabolic syndrome: a cross-sectional cohort study. Diabetol Metab Syndr 7: 3.
- World Health Organization (1998) Obesity: Preventing and managing the global epidemic. Report of a WHO Consultation on Obesity.
- Wu JT, Wu LL (2006) Linking inflamation and atherogenesis: Soluble markers identified for the detection of risk factors and for early risk assessment. Clin Chim Acta 366(1-2): 74-80.
- Yudkin JS, Stehouwer CDA, Emeis JJ, Coppack SW (1999) C-reactive protein in healthy subjects: associations with obesity, insulin resistance, and endotelial dysfunction: a potencial role for cytokines originating from adipose tissue? Arterioscler Thromb Vasc Biol 19: 972-978.
- Ziegler O (2001) Hyperthiglycéridémies et risque vasculaire. Objectif Nutr.
