 Research Article
Research ArticleAbstract
Objective: To estimate the burden of pneumonia (PNM) mortality in the elderly in Brazil using different methodologies for rate correction.
Method: A time-series study of mortality rates from PNM in the elderly from 2005- 2016. For the correction of the rates, two strategies were used: 1-correction by active search (CBA) and 2-correction by active search more redistribution (CBAR). In addition, a methodology for comparing corrected rates, calculated lower respiratory tract infection rates (ITRi) using estimates from the Global Burden Disease study. Trend was assessed using regression models.
Result: From 2005 to 2016, 546,068 deaths were registered, which, after using the CBAR correction strategy, left 501,380, a reduction of 8.2%. There was an increasing trend of PNM mortality rates for all regions of Brazil and for the elderly population. The largest linear increase in mortality rate due to CBAR pneumonia was observed in the Northeast.
Conclusion: These estimates of the magnitude and trend presented make it possible to analyze the behavior of mortality rates due to pneumonia in the elderly in Brazil and to subsidize the National Immunization Program on the need to include a specific pneumococcal vaccine for the entire elderly population.
Keywords: Mortality Registries; Mortality Systems Integration; Under Registration; Pneumonia; Aged
Abbreviations: CBA: Correction by Active Search; CBAR: Correction by Active Search Plus Redistribution; DO: Death Certificate; GBD: Global Burden of Diseases Project; GC: Garbage Codes; IBGE: Brazilian Institute of Geography and Statistics; ICD-10: 10th edition of the International Statistical Classification of Diseases and Related Health Problems; IHME: Institute of Metrics and Assessment in University of Washington Health in Seattle; ITRi: Lower Respiratory Tract Infection; MS: Ministry of Health; PNM: Pneumonia; SC: Without Correction; SIH: Hospital Information System; SIM-SUS: Mortality Information System of the Unified Health System; SIM: Mortality Information System; SUS: Unified Health System; UF: Federation Units
Introduction
Since the beginning of the use of mortality data, which occurred
in England in the middle of the 16th century, the information has
enabled the construction of indicators that can characterize the
epidemiological profile of a population. Fact that contribute to
monitor health conditions and support the implementation of public
health interventions targeted at a specific population. In Brazil, the
Mortality Information System (SIM), implemented in 1975, has
accumulated, over time, improvements in its performance, both
in increasing its coverage and in the quality of information on the
cause of death [1-3]. This improvement is possible due to the efforts
made by SIM managers at different levels of performance. However,
this work has a high cost and requires qualified professionals [4]. It
is observed that there are still quality problems in the registration
of the basic cause of death in the Death Certificate (DO), with high
percentages of little useful codes (garbage codes - GC), registered
as the basic cause of death [5]. These GC are contained in the
various chapters of the 10th edition of the International Statistical
Classification of Diseases and Related Health Problems (ICD-10)
[6].
In addition, another problem is the lack of completeness of the
information in variables present in the DO. Common examples of
incorrect completion of the DO are statement not of the underlying
cause but of its consequence; or just the commitment of a specific
organ or system; or even the generic name of the disease, without
the necessary specifications, among other examples [4,7]. Some
strategies were implemented by the Ministry of Health (MS) in order
to reduce the underreporting of deaths in the SIM and improve the
quality of filling in the cause of death. The following stand out:
a) The research “Active Search for Deaths and Births” [8],
whose purpose was to assess the underreporting of deaths in
the SIM;
b) The project to reduce ill-defined causes (chapter XVIII of
ICD-10);
c) The project to reduce the less useful GC codes [8,9],
linking mortality data with the hospitalization information
system; and
d) Implantation of verbal autopsy forms for deaths without
medical assistance.
These initiatives have been successful in terms of improving SIM
coverage and also in the significant reduction of GC in chapter XVIII
of ICD-10, but the challenge of reducing the other CG in the other
chapters of ICD-10 remains, especially the causes not specified
within the chapters. Currently, an intervention project is underway
with medical professionals in large hospitals in the metropolitan
regions of the country with the aim of qualifying the completion of
the DO, in order to reduce the percentage of GC [2].
Advances in the SIM computerized system, together with
improved coverage and quality of information, have enabled the
development of research using its databases. The use of linkage
between databases is a good example of this evolution. This
technique allows to qualify the data of the information system when
relating the same individual to another information system, such
as, for example, the Hospital Information System (SIH), which is
responsible for processing and registering all hospital admissions
financed by the Unified Health System in Brazil (SUS) [4,10,11].
A recent study that used the linkage strategy between these two
databases made it possible to identify the hospital admission
diagnoses in the SIH of individuals with pneumonia (PNM) as the
cause of death in the SIM. The result of the study made it possible
to reclassify 17.4% of the causes in which the PNM was considered
a basic cause in the SIM to other causes of death [10]. However,
even with the adoption of these strategies, it is possible that the
true burden of PNM in Brazil is still unknown. Based on these
limitations, this research aimed to estimate the burden of mortality
due to PNM in the elderly in Brazil using different rate correction
methodologies.
Materials and Methods
Ecological study of time series based on the death records of the Mortality Information System of the Unified Health System (SIM-SUS) in Brazil, between the years 2005 and 2016. All deaths occurred in the elderly aged 60 years or older were selected age and who had, as a basic cause, PNM (ICD-10: J12-J18). Estimates of the resident population by regions of Brazil (Central-west, Northeast, North, Southeast and South), according to age group (60-64, 65- 79 and 80 years or older) in the study period (2005-2016) were obtained through exponential interpolation of the population of the 2000 and 2010 censuses, for the first of July, released by the Brazilian Institute of Geography and Statistics (IBGE). The 2000 and 2010 census estimates available on the IBGE online platform were considered [12]. Mortality rates for PNM without correction (SC) per 100 thousand inhabitants were calculated using the number of deaths registered in the SIM as a numerator and the resident population for the same region, age group and period, as the denominator. To correct the rates, two strategies were used: 1-correction by active search (CBA) and 2-correction by active search plus redistribution (CBAR).
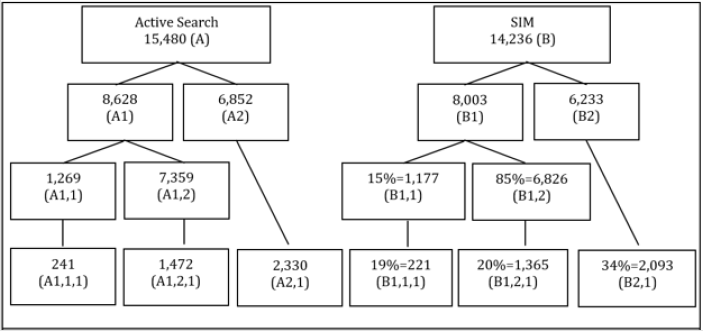
Figure 1: Example of the strategy used to calculate the CBA factor for pneumonia in 60 years or older in the South in 2005.
A: Number of deaths of Chapter X (ICD-10) of Active Search with 60 years or older
A1: Number of deaths of Chapter X (ICD-10) of the Active Search from 60 to 79 years
A2: Number of deaths in Chapter X (ICD-10) of Active Search with 80 years or older
A1,1 = A1*B1,1: Estimated number of deaths in Chapter X (ICD-10) of Active Search from 60 to 64 years
A1,1,1 = A1,1*B1,1,1: Estimated number of deaths from active search pneumonia from 60 to 64 years
A1,2 = A1*B1,2: Estimated number of deaths in Chapter X (ICD-10) of Active Search from 65 to 79 years
A1,2,1 = A1,2*B1,2,1: Estimated number of deaths from active search pneumonia from 65 to 79 years
A2,1 = A2*B2,1: Estimated number of deaths from active search pneumonia aged 80 and over
B: Number of deaths in Chapter X (ICD-10) registered in SIM aged 60 years or older
B1: Number of deaths in Chapter X (ICD-10) registered in the SIM from 60 to 79 years
B2: Number of deaths in Chapter X (ICD-10) registered in SIM aged 80 years or older
B1,1: Proportion of deaths in Chapter X (ICD-10) registered in SIM from 60 to 64 years
B1,1,1 = Proportion of deaths from pneumonia registered in the SIM from 60 to 64 years
B1,2: Proportion of deaths in Chapter X (ICD-10) registered in the SIM from 65 to 79 years
B1,2,1: Proportion of deaths due to pneumonia registered in the SIM from 65 to 79 years
B2,1: Proportion of deaths due to pneumonia registered in SIM aged 80 years or older
CBA factor 60 to 64 years = A1,1,1/B1,1,1 = 1.08
CBA factor 65 to 79 years = A1,2,1/B1,2,1 = 1.08
CBA factor 80 years or older = A2,1/B2,1 = 1.10.
In the construction of the first strategy, CBA, the number of
deaths underreported by PNM was estimated for the age groups
of the study. In calculating the number of deaths by age group 60-
64 years and 65-79 years, a proportion based on the age group
60-79 years of the active search research was used [8]. The same
condition was adopted for the proportion of PNM (ICD-10: J12-J18)
underreported in relation to deaths from diseases of the respiratory
system (chapter X - ICD-10). These estimates were based on the
number of deaths reported in the SIM. From the estimate of the
number of deaths underreported by PNM for the period (2005 to
2013), by age group (60-64 years, 65-79 years and 80 years or
older) by regions of Brazil, it was possible to calculate the risk factor
CBA for the years 2005 to 2013. Figure 1 exemplifies this strategy
carried out for the South region in 2005. In a complementary way, the linear regression model was adopted to project the CBA factor
from 2014 to 2016. This annual correction was applied to the SC
rates.
The second strategy, which is a correction factor for PNM
mortality data recorded in SIM, was carried out based on the
results of the study on the redistribution of the basic cause of
death using data matching between SIM and SIH-SUS from 2008 to
2013 [10]. The ICD-10 codes registered in the primary diagnosis
field (or secondary diagnosis, only in the case of external causes)
of the AIH were used to review the basic cause of death, taking
into account the diagnoses of hospitalization SIH other than PNM.
For this redefinition of the basic cause of death, the diagnosis of
hospitalization was inserted in lines A, B, C and D of part I of the
DO, where the causes that led to death are recorded, preserving the
causes registered in the original DO. After inserting the diagnosis
of hospitalization in the DO, the basic cause was redefined using
the SIM Basic Cause Selector software. After this process, the PNM
correction factor was defined as the basic cause of death for the
years 2008 to 2013. The linear regression model was performed
to estimate the correction factor for the other years: 2005 to 2007
and 2014 to 2016. This second correction strategy was called CBAR.
In defining the estimated mortality rate, deaths corrected
by the two strategies described above, active search and active
search plus the redistribution of the underlying cause, were used
as numerators. Additionally, as a reference or parameter for the
mortality rates estimated by the study, we used the estimates of
deaths due to lower respiratory tract infection (ITRi) produced
by the Global Burden of Diseases Project (GBD), from the Institute
of Metrics and Assessment in University of Washington Health in
Seattle (IHME). In defining this new mortality rate in the elderly,
the deaths estimated by GBD were used as a numerator in the group
of causes of death due to ITRi using the estimates of the GBD study
[13]. The estimate by brazilian regions was possible due to the
cooperation agreement between the MS of Brazil and the IHME for
the production of the GBD indicators for the Federation Units (UF).
GBD methodological details are available in other publications of
the group, which updates its procedures and concepts since the
first publication [14].
As GBD’s estimates of the number of deaths by ITRi (ICD-10:
A48,1, A70, J09-J15,8, J16-J16,9, J20-J21,9 and P23,0-P23,4) are
available on the IHME online page by UF in Brazil, by year and by
age group, the number of deaths by region was calculated from the
sum of the UF [15]. Thus, the GBD mortality rate was calculated
by adopting, as a numerator, the death estimate by ITRi; and, as a
denominator, the same population previously described, by region,
age group and year. For the analysis of the trend of mortality due
to SC pneumonia, CBA, CBAR and ITRi-GBD, dispersion diagrams
between the coefficients and the years of study were made in order
to visualize the function that could be expressing a relationship
between them. From this relationship, it was possible to choose the
simple linear regression model (Y = β0 + β1X), which, in addition to
its statistical power, allows to define a forecast function [16]. In this
model, β0 is the average annual coefficient and β1 is the coefficient
of linear effect (speed). For modeling, the mortality coefficients
were considered as a dependent variable (Y axis) and the years of
the study series as an independent variable (X axis).
For the adjustments of these models, classic assumptions were
verified, such as normality, independence and homoscedasticity of
the residues [16]. The Durbin-Watson test was used to observe the
autocorrelation between the residues. It was adopted as a measure
of precision of the model the use of the coefficient of determination
(R2). A significant trend was considered as one whose estimated
model obtained a significant regression coefficient (p <0.05). The
study was carried out in compliance with the ethical precepts of
Resolution 466, of December 12, 2012 [17], and, after its approval
by the Research Ethics Committee of the Federal University of Goiás
- whose number is 162,532. Due to the fact that the use of data from
a large national database is foreseen without the identification
of the research subjects, there was no need to use the Informed
Consent Form.
Results
In the period from 2005 to 2016, 546,056 deaths in the elderly
were registered in the SIM in Brazil, with the primary cause of PNM.
After applying the correction factor (CBAR), 501,380 records were
considered as PNM, which corresponds to an 8.2% reduction in
deaths with PNM registration as the basic cause in the period. Table
1 and Figures 2-4 show mortality rates due to PNM in the elderly
without correction and those corrected during the study series.
Differences were found between the adopted methodologies.
The temporal evolution of mortality rates by PNM CBAR showed
an increasing trend for all geographic regions of Brazil and age
group in the period between 2005 and 2016 (Tables 1), (Figures
2-4). These also show mortality rates from ITRi-GBD with regional
variations. There is a progressive increase in mortality rates due to
PNM with advancing age, with higher risks in the age group of 80
years or older.
In 2016, the Southeast region had the highest mortality
rate by PNM (1,245.55/100,000 inhab.), Followed by the North
(1,074.09/100,000 inhab.), Central-west (965.35/100,000 inhab.),
Northeast (943.64/100,000 inhab.) and South (881.96/100,000
inhab.). Figures 2-4 present the results in graph form. The number
of deaths from PNM without correction, from different correction
strategies and from ITRi by GBD are shown in Table 2. The
linear regression model Table 3. shows an increase in the linear
component (B1) for all age groups, the longer the age group, the
greater the magnitude of the annual increase. The Northeast region
showed the largest linear increase in the mortality rate due to CBAR
pneumonia for the age groups 60-64, 65-79 and 80 years or older. The smallest linear increase was observed in the Central-west and
South regions, in the age group 60-64 years, and in the age group 80
years or older for the South region.
Table 1: Annual rates (per 100,000) uncorrected and corrected for pneumonia mortality and ITRi by GBD by age group, region and year. Brazil, 2005-2016.
Note: PNM-SC rate: Pneumonia rate without correction; PNM-CBA rate: Pneumonia rate corrected by the active search survey; PNM-CBAR rate: Pneumonia rate corrected by research on active search and reassignment; ITRi-GBD Rate: Global Burden Disease infection rate of the lower respiratory tract.
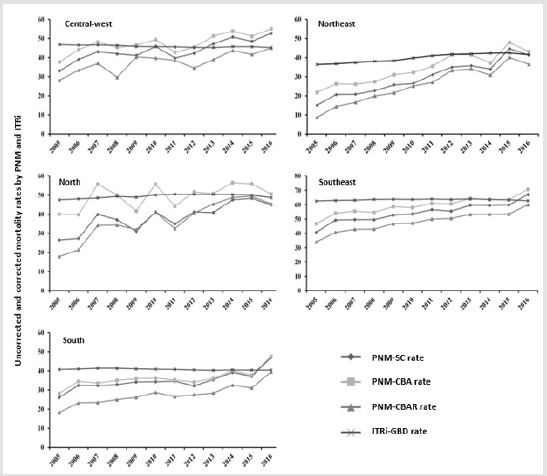
Figure 2: Trend of rates (per 100,000) uncorrected and corrected for mortality from pneumonia and lower respiratory tract infection in elderly aged 60 to 64 years by region. Brazil, 2005 - 2016.
Note: PNM-SC rate: Pneumonia rate without correction; PNM-CBA rate: Pneumonia rate corrected by the active search survey; PNM-CBAR rate: Pneumonia rate corrected by research on active search and reassignment; ITRi-GBD Rate: Global Burden Disease infection rate of the lower respiratory tract.
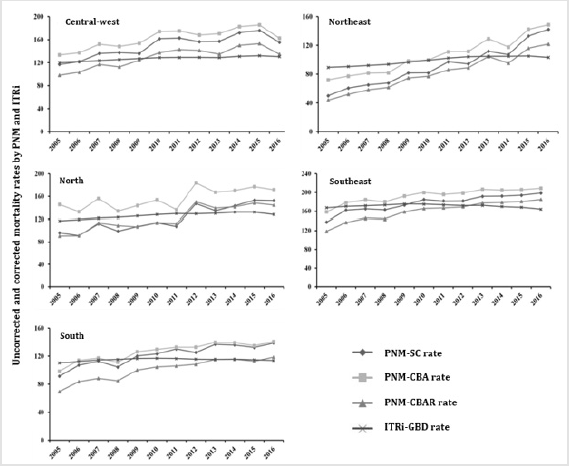
Figure 3: Trend of rates (per 100,000) uncorrected and corrected for mortality from pneumonia and lower respiratory tract infection in elderly aged 65 to 79 years by region. Brazil, 2005 - 2016.
Note: PNM-SC rate: Pneumonia rate without correction; PNM-CBA rate: Pneumonia rate corrected by the active search survey; PNM-CBAR rate: Pneumonia rate corrected by research on active search and reassignment; ITRi-GBD Rate: Global Burden Disease infection rate of the lower respiratory tract.
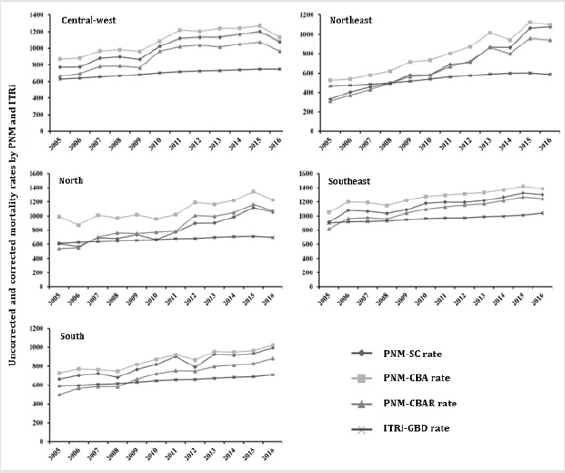
Figure 4: Trend of rates (per 100,000) uncorrected and corrected for mortality from pneumonia and lower respiratory tract infection in elderly aged 80 years or older by region. Brazil, 2005 - 2016.
Note: PNM-SC rate: Pneumonia rate without correction; PNM-CBA rate: Pneumonia rate corrected by the active search survey; PNM-CBAR rate: Pneumonia rate corrected by research on active search and reassignment; ITRi-GBD Rate: Global Burden Disease infection rate of the lower respiratory tract.
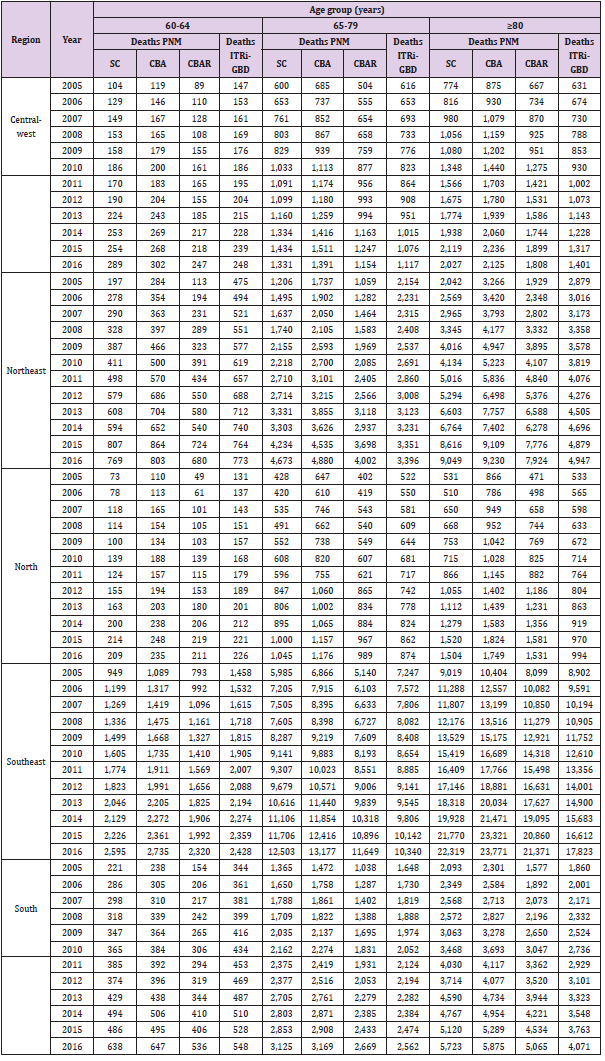
Table 2: Number of deaths without correction and corrected by pneumonia and ITRi by GBD by age group of elderly, region and year. Brazil, 2005-2016.
Note: Deaths PNM-SC: Number of deaths from pneumonia without correction; Deaths PNM-CBA: Number of deaths from pneumonia corrected by the search for active search; Deaths PNM-CBAR: Number of deaths from pneumonia corrected by the search for active search and redistribution; Deaths ITRi-GBD: Number of deaths due to infection of the lower respiratory tract by Global Burden Disease.
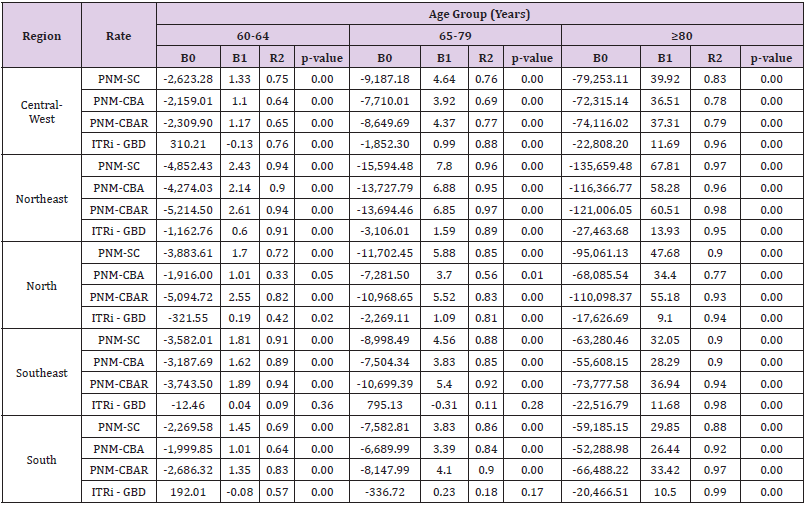
Table 3: Adjustments of the linear regression model for annual rates (per 100.000) without correction and corrected for mortality from pneumonia and ITRi by GBD by age group. region and year. Brazil. 2005-2016.
Note: PNM-SC rate. Pneumonia rate without correction; PNM-CBA rate. Pneumonia rate corrected by the active search survey; PNM-CBAR Rate. Pneumonia rate corrected by the search for active search and redistribution; ITRi-GBD Rate. Global Burden Disease infection rate of the lower respiratory tract
Discussion
The main results of this study were
a) Estimation of mortality rates due to PNM, using correction
methods for underreporting deaths [8] and the basic cause of
death [10]; and
b) The analysis of the trend in mortality rates due to PNM in
the elderly by regions and age group.
There was a progressive increase in mortality rates due to
PNM in elderly people in Brazil directly proportional to age;
it was also possible to describe the differences between the
geographic regions of the country.
Brazil is a country of continental dimensions and important
social and economic differences in each region [18,19]. In this
study, the Northeast region, followed by the North, were those
that showed the highest increase in the mortality rate due to CBAR
pneumonia in all age groups. In this sense, research has shown
that these two regions present disparities in the indicators of
education, material deprivation and use of health services when
compared to the others [19]. Recent national research on the trend of mortality due to PNM in Brazil also lists the Northeast and North
regions as being disparate in relation to the others [20]. There is
no doubt that the increase in investment in public policies aimed
at vaccination is associated with the relevant reduction in general
and specific mortality due to PNM and influenza, as well as the
reduction of health inequities in the country [21]. An important
result of this study was the identification of a tendency to increase
the magnitude of mortality rates due to PNM in elderly people in
Brazil in all regions of the country, in the period from 2005 to 2016.
This increase in mortality was directly proportional to the
increase in the age group of the elderly. Studies have shown an
increasing trend both in mortality [20] and in morbidity due to PNM
in the elderly in Brazil, even after the implementation of intervention
strategies [22]. With advancing age, in addition to increasing
exposure to environmental factors, the body’s defense mechanisms
reduce the ability to fight pathogenic microorganisms, increasing
susceptibility to communicable diseases (immunosensitivity or
immune aging), which is aggravated by the multicomorbidities
present in this age group [6,7,23-25]. Such an assertion may be
associated with the increase in mortality rates in elderly people
aged 80 years or older observed in this research. This increase
is in contrast to what has been observed in other countries that
implanted conjugated pneumococcal vaccination for children
longer than in Brazil, in addition to having also implemented it
for adults [23,26,27]. Although in these countries the number of
deaths due to ITRi in the elderly is higher than in other age groups,
mortality rates have been decreasing.
The main speculation is that it is associated with the effect
of herd immunization and also with vaccination in the elderly
themselves [23,26]. Until the completion of this study, the 23-valent
polysaccharide vaccine was available only in private clinics, with
limited access to the elderly with greater purchasing power.
The vaccine is only available free of charge for special groups of
hospitalized elderly and/or residents of long-term care facilities,
as well as for people with chronic and immunodepressed diseases
[28]. There is a need to direct efforts to increase the availability of
the vaccine to all the elderly in the country. Despite the important
improvement in the coverage and quality of the information
contained in the SIM [2,3,29], there are still regional inequalities
in terms of filling the causes of death in the DO, which makes it
difficult to know the ‘true’ burden of PNM in the Brazil. In addition,
it is important to emphasize errors in filling out and coding the
causes of death in DO. These are observed, more frequently, in the
elderly population due to the multiple comorbidities presented that
make it difficult to define the real basic cause of death [6,7,23].
Part of the deaths registered as PNM are, in fact, an associated
cause or do not represent the basic cause of death [6,30,31]. A study
carried out in 2010 in Brazil reclassified 65.5% of ill-defined causes
[3]. Another study redistributed 67% of the cases of neoplasms
after applying linkage between databases [32]. In 2018, a study
redistributed 17.4% of the cases in which PNM was considered a
basic cause of death [10]. Still in that same study, after applying
the strategy to redistribute the basic cause of death, the mortality
rate due to PNM in Brazil reduced seven deaths per 100,000
inhabitants. In particular, the study presented here adopts CBAR
strategies, correction of under enumeration and overestimation
of deaths, as a more appropriate estimate of the burden of PNM in
the elderly population for Brazil. The use of these two strategies
allowed to know more robust estimates of mortality rates due to
PNM in the elderly in Brazil, which contributed to the reduction of
garbage codes.
The use of ITRi-GBD rates served as a parameter to compare
two proposed correction methodologies: CBA and CBAR. Although a
previous study showed an increase in both the number of deaths and
mortality rates due to ITRi in the population aged 70 years or older
[33], in this research the trend of ITRi-GBD rates showed a more
stable behavior during the series when compared with CBAR rates.
The correction factors used by the GBD methodology to project the
rates appear to be much higher at the beginning when compared to
the end. This fact can be seen in the improvement in the quality of
SIM data in recent years [2,3,29]. There are several actions taken
by the MS and by the state and municipal health secretariats, in
partnership with universities, in order to reduce problems related
to the coverage and inadequate filling of causes of death in DO,
mainly errors of diagnosis of the basic cause of death [2,3,8,34]. An
important action taken was the research named “Active Search for
Deaths and Births” and the Project to Reduce Ill-Defined Causes of
Death, which managed to reduce the under-registration of deaths
and the percentage of causes of death codified in chapter XVIII of
the ICD- 10 [8,9].
The adoption of this strategy, CBA, has already been applied in
other studies with the same purpose, which is to correct the underregistration
and bring it closer to values closer to the real [7,35].
But in this study, we corrected in addition to the under-registration
the coding errors of the basic cause. Another aspect that should
be emphasized is the lesser protection of the herd conferred by
infant 10-valent pneumococcal vaccination in the extreme elderly,
in addition to the low effectiveness of the vaccine for disease
prevention in the elderly when compared to young adults. It is also
important to highlight the increase in the circulation of non-vaccine
serotypes in this population [36].
This study enabled estimates closer to the reality of mortality
rates due to PNM in the elderly in the five regions of Brazil, since
both the under-registration correction (CBA) was adopted, which
in theory would increase the number of notifications, as well as
errors codification through the redistribution of deaths by PNM to
other causes. The main limitations of the study were the presence
of a certain degree of uncertainty in the estimated rates, even after using the proposed methodology. The additional use of basic cause
redistribution research may present limitations related to possible
biases that may have occurred in the database linkage process, such
as different patterns of cause of death between cases that were
paired and not paired [10]. Despite the limitations listed when
using data from the MS information systems, it is believed that the
technique proposed in this study represents a viable and adequate
alternative for estimating the mortality burden of PNM in the
elderly. In addition, studies that include validation and reliability
strategies for improving methodologies to correct information on
the basic cause of death are necessary and should be encouraged
to improve the SIM.
Conclusion
This study proposed and used methodologies to correct the mortality rate due to PNM in Brazil that can be applied in analyzes for other groups of causes. The results showed that in 2016 there were more risks of mortality from PNM in the Southeast and North regions; and that the trends of increase in mortality rates due to PNM in elderly people aged 60 years or older in Brazil, with higher rates of increases, were in the Northeast and North regions of the country. The magnitude and trend estimates presented in the study make it possible to analyze the behavior of mortality rates due to PNM in the elderly in Brazil. In addition, they can subsidize the National Immunization Program on the need to include a specific pneumococcal vaccine for the entire elderly population.
Acknowledgement
To the National Council for Scientific and Technological Development (CNPq), for granting a doctoral scholarship to the first author.
Conflict of Interest
The authors have declared that no competing interest exists.
Author’s Contribution
DBM, ALA and OLMN worked on the conception and design of the research, the analysis and interpretation of data, the writing of the article and the approval of the version to be published. GMP, RM and ALB worked on data analysis and interpretation, writing the article and approving the version to be published.
References
- Frias PG, Szwarcwald CL, Morais OL, Leal MC, CortezEscalante JJ, et al. (2017) Use of vital data to estimate mortality indicators in Brazil: from the active search for events to the development of methods. Cad Saude Publica 33(3): e00206015.
- Souza MFM, França EB, Cavalcante A (2017) Burden of disease and health situation analysis: results of the Global Burden of Disease (GBD) Brazil network. Rev Bras Epidemiol1(Suppl 1): 1-3.
- França E, Teixeira R, Ishitani L, Duncan BB, CortezEscalante JJ, et al. (2014) Ill-defined causes of death in Brazil: a redistribution method based on the investigation of such causes. Rev. Saude Publica 48(4): 671-81.
- Jorge MHPM, Cascão ÂM, Reis AC, Laurenti R (2012) In search of better information on the basic cause of death through linkage: a snapshot on external causes in the elderly - State of Rio de Janeiro, Brazil, 2006. Epidemiology and Health Services 21(3): 407-418.
- Naghavi M, Makela S, Foreman K, O’Brien J, Pourmalek F, et al. (2010) Algorithms for enhancing public health utility of national causes-of-death data. Popul Health Metr 8: 9.
- Ishitani LH, Teixeira RA, Abreu DMX, Paixão LMMM, França EB (2017) Quality of mortality statistics’ information: garbage codes as causesof death in Belo Horizonte, 2011-2013. Rev Bras Epidemiol 1(Suppl 1): 34-45.
- Jorge MHPDM, Laurenti R, Lima-Costa MF, Gotlieb SLD, Filho ADPC (2008) Elderly mortality in Brazil: the question of ill-defined causes. Epidemio. and Health Services17(4): 271-281.
- (2018) DATASUS. Health information. Correction and redistribution of deaths according to the active search survey. Ministry of Health of Brazil.
- Szwarcwald CL, Neto OLM, Frias PG, Junior PRBS, Cortez JJE, et al (2011) Active search for deaths and births in the Northeast and the Legal Amazon: Estimation of SIM and Sinasc coverage in Brazilian municipalities. In: Ministry of Health of Brazil, Health Brazil 2010: an analysis of the health situation and selected evidence of the impact of health surveillance actions, Brasília p. 79-98.
- Policena GM (2018) Redistribution of the underlying cause of deaths from pneumonia in adults by matching hospitalization and mortality records, Brazil, 2008-2013. Goiânia, Federal University of Goiá
- Cascão AM, Jorge MHPM, Costa AJL, Kale PL (2016) Use of primary diagnosis during hospitalization in the Unified Health System (Sistema Único de Saúde) to qualify information regarding the underlying cause of natural deaths among the elderly. Rev Bras Epidemiol 19(4): 713-726.
- (2018) Brazilian Institute of Geography and Statistics of Brazil. Statistic. Brazilian census.
- GBD 2015 Disease and Injury Incidence and Prevalence Collaborators (2016) Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 388(10053): 1545-1602.
- Murray CJL, Lopez AD (1996) The global burden of disease: a comprehensive assessment of mortality and disability from deceases, injuries and risk factors in 1990 and projected to 2010. Harvard Univ Press 1(1): 1-35.
- (2018) Institute for Health Metrics and Evaluation. GBD Compare.
- Latorre MRDO, Cardoso MRA (2001) Analysis of time series in epidemiology: an introduction to methodological aspects. Rev Bras Epidemiol4(3): 145-152.
- (2012) Ministry of Health of Brazil. National Health Council. Resolution no. 466 of December 12, 2012, Brasilia.
- Vasconcelos AMN, Gomes MMF (2012) Demographic transition: the Brazilian experience. Epidemiol e Serviços Saúde 21(4):539-548.
- Szwarcwald CL, Souza PRB, Marques AP, Almeida WDS, Montilla DER (2016) Inequalities in healthy life expectancy by Brazilian geographic regions: findings from the National Health Survey, 2013. Int J Equity Health 15(1):141.
- Ferraz RO, Oliveira-Friestino JK, Francisco PMSB (2017) Pneumonia mortality trends in all Brazilian geographical regions between 1996 and 2012. J Bras Pneumol 43(4):274-279.
- Antunes JLF, Waldman EA, Borrell C, Paiva TM (2007) Effectiveness of influenza vaccination and its impact on health inequalities. Int J Epidemiol 36(6): 1319-1326.
- Andrade AL, Afonso ET, Minamisava R, Bierrenbach AL, Cristo EB, et al. (2017) Direct and indirect impact of 10-valent pneumococcal conjugate vaccine introduction on pneumonia hospitalizations and economic burden in all age-groups in Brazil: A time-series analysis. PLoS One 12(9): e0184204.
- Lexau CA, Lynfield R, Danila R, Pilishvili T, Facklam R, et al. (2005) Changing epidemiology of invasive pneumococcal disease among older adults in the era of pediatric pneumococcal conjugate vaccine. JAMA 294(16):2043-2051.
- Almirall J, SerraPrat M, Bolibar I (2016) Risk Factors for Community-acquired Pneumonia in Adults: a review. Clin Pulm Med 23(3):99-104.
- Almirall J, SerraPrat M, Bolíbar I, Balasso V (2017) Risk Factors for Community-Acquired Pneumonia in Adults: A Systematic Review of Observational Studies. Respiration 94(3):299-311.
- Harboe ZB, Dalby T, Weinberger DM, Benfield T, Mølbak K, et al. (2014) Impact of 13-valent pneumococcal conjugate vaccination in invasive pneumococcal disease incidence and mortality. Clin Infect Dis 59(8): 1066-1073.
- Bonten MJM, Huijts SM, Bolkenbaas M, Webber C, Patterson S, et al. (2015) Polysaccharide conjugate vaccine against pneumococcal pneumonia in adults. N Engl J Med 372(12):1114-1125.
- (2014) Ministry of Health of Brazil. Manual of reference centers for special immunobiologists. Brasilia.
- Phillips DE, Lozano R, Naghavi M, Atkinson C, GonzalezMedina D, et al. (2014) A composite metric for assessing data on mortality and causes of death: the vital statistics performance index. Popul Health Metr 12:14.
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, et al. (2012) Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380(9859):2095-2128.
- Sgambatti S, Minamisava R, Afonso ET, Toscano CM, Bierrenbach AL, et al. (2015) Appropriateness of administrative data for vaccine impact evaluation: the case of pneumonia hospitalizations and pneumococcal vaccine in Brazil. Epidemiol Infect 143(2): 334-342.
- Oliveira PPV, Silva GA, Curado MP, Malta DC, Moura L (2014) Reliability of cancer as the underlying cause of death according to the Mortality Information System and Population-Based Cancer Registry in Goiânia, Goiás State, Brazil. Cad Saude Publica 30(2): 296-304.
- Corrêa RA, José BPS, Malta DC, Passos VMA, França EB, et al (2017) Burden of disease by lower respiratory tract infections in Brazil, 1990 to 2015: estimates of the Global Burden of Disease 2015 study. Rev Bras Epidemiol 1(Suppl 01):171-181.
- Batista Filho M, Cruz RSBLC (2015) Children's health in the world and in Brazil. Rev Bras Maternal Health Infant 15(4): 451-54.
- Almeida WS, Szwarcwald CL (2017) Adequacy of mortality data and correction of reported deaths from the Proactive Search of Deaths. Cien Saude Colet 22(10):3193-3203.
- Christophe BL, Mott M, Cunha G, Caierão J, Azevedo PD, et al. (2018) Characterisation of Streptococcus pneumoniae isolates from invasive disease in adults following the introduction of PCV10 in Brazil. J Med Microbiol 67(5): 687-694.
